
In this ECG Cases blog we review an approach to tachycardia, explore the WIDER mnemonic for wide SVT differential diagnosis, and how to distinguish VT from SVT with 10 cases…
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. March 2021
10 patients presented with tachycardia. What’s the diagnosis and management?
Case 1: 25yo found confused with an empty bottle of pills. HR 130 BP 150/90 R20 sat 97% temp 38.0
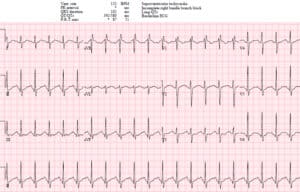
Case 2: 75yo with sudden palpitations. HR 210 BP 110/70 R18 sat 98%

Case 3: 80yo CAD with 2hr chest pressure. HR 130 BP 120/70 R24 sat 95%. Old then new ECG


Case 4: 80yo DM/HTN with few days weakness. HR 105 BP 120/80 R18 sat 97%

Case 5: 70yo with few days of weakness, not eating. HR 120 BP 120/75 R20 sat 96%. Serial ECGs


Case 6: 75yo admitted with anterior STEMI 5 days prior, sudden collapse, pulseless

Case 7: 75yo with acute SOB and diaphoresis. HR130, BP 100/80 R24 sat 89%

Case 8: 60yo acute chest pain. HR 125 BP 90/60 R24 sat 90%

Case 9: 25yo sudden palpitations. HR 150 BP 120/80 R18 sat 99%

Case 10: 60yo CAD with SOB and chest pressure. HR 180 BP 80/60 R20 sat 92%

An Approach to Tachycardias
The management of tachycardia (HR>100 in adults) depends on the ECG and the patient:
- Sinus tachycardia (P waves before every QRS, upright in in I and II): treat underlying cause
- Unstable
- from non-sinus tachycardia: electrical cardioversion
- unrelated to non-sinus tachycardia: treat underlying +/- rate/rhythm
- Stable non-sinus tachycardia
- Narrow QRS (<120ms)
- Irregular
- Different P wave morphologies = MAT: treat underlying, magnesium
- Flutter waves = atrial flutter with variable block: treat underlying, rate/rhythm control
- No P/flutter waves = atrial fibrillation: treat underlying, rate/rhythm control
- Regular
- Flutter waves = atrial flutter with fixed block: treat underlying, rate/rhythm control
- No preceding P/flutter waves = SVT: vagal, adenosine, CCB, cardiovert
- Irregular
- Wide QRS (>120ms)
- Irregular
- Afib/flutter with BBB: treat underlying, rate/rhythm control
- AF + WPW: procainamide, electrical cardioversion
- Polymorphic VT: electrical cardioversion, amiodarone if normal QT, magnesium if long QT
- Regular: monomorphic VT vs SVT: adenosine, procainamide, electrical cardioversion
- Irregular
- Narrow QRS (<120ms)
The first step is to identify sinus tachycardia because the management—whether the patient is stable or unstable, and whether the QRS is narrow or wide—is to identify and treat the underlying cause. Because P waves are small and can be confused with T waves, U waves, flutter waves or artifact, computer interpretation often fails at rhythm analysis [1]. But remembering anatomy can help: sinus conduction begins in the upper right atrium and spreads down and to the left, so look at V1 for biphasic P waves and lead II for upright P waves.
If the tachycardia is not sinus, then the next step is to assess clinical stability and consider electrical cardioversion. If a patient is clinically unstable as a result of non-sinus tachycardia, then the management—whether narrow complex like SVT or AF, or wide complex like VT or SVT with abberancy—is immediate electrical cardioversion. On the other hand, a patient’s instability might be unrelated to their tachycardia (eg chronic atrial fibrillation with hypotension from sepsis), requiring treatment of the underlying cause with or without managing their arrhythmia.
If the patient has a non-sinus tachycardia but is stable, then further analysis of the ECG can identify the specific arrhythmia and guide management—based on QRS width, regularity and atrial activity. Narrow complex tachycardia (QRS<120ms) indicates normal ventricular conduction and therefore a supraventricular source of arrhythmia. As with sinus rhythm, leads V1 and II are helpful to identify flutter waves, which most commonly proceed in a counter-clockwise loop away from lead II (producing inverted flutter waves) and towards V1 (producing upright flutter waves mimicking P waves). Wide complex tachycardia (QRS>120) can be either supraventricular (with abnormal conduction, from a variety of possible reasons) or ventricular in origin. As a review article summarized, “A large body of discussion has focused on the 2 major types of WCT: ventricular tachycardia (VT) and paroxysmal supraventricular tachycardia (PSVT) with aberrancy. However, there are several other important causes of a WCT encountered in clinical practice, which are less often discussed. These tachycardias are abnormal, often requiring specific therapies differing from the standard approach to WCT.”[2] The differential for supraventricular rhythms that have wider QRS complexes can be remembered by the mnemonic WIDER.
WIDER Mnemonic for DDx SVT with Wide QRS
- WPW + AF: very rapid, irregular and variable complexes: procainamide or electrical cardioversion
- Intraventricular conduction delay: pre-existing or rate-related BBB: treat underlying
- Drugs: sodium channel blocker (sinus tach, QRS>100 and possibly very wide, right axis, tall R in aVR): sodium bicarb
- Electrolytes: hyperkalemia (long PR or junctional rhythm, prolonged QRS, peak T, “slow VT” or “very wide VT”): calcium, glucose/insulin
- Raised ST segments (STEMI) producing pseudo-QRS widening: reperfusion
If the differential is narrowed down to VT vs SVT with aberrancy, there’s an 80% pre-test likelihood of VT, even higher in older patients with CAD. There are certain criteria that can further suggest VT—based on VT originating in the ventricles independently of the atria, and propagating through delayed conduction in an abnormal direction:
- Heart rate/rhythm: AV dissociation, caption/fusion beats
- Electrical conduction:
- prolonged conduction: QRS>140, RS>100, R-wave peak>50ms in lead II
- morphology
- Atypical LBBB: V1 r>30ms, RS>60, notched S; V6 Q wave
- Atypical RBBB: V1 monophasic R or R>R’; V6 R:S<1
- Axis: extreme axis deviation, axis change from baseline
- R-wave: precordial concordance (all precordial leads have either positive concordance or negative concordance); absence of RS complex in precordial leads; monophasic R in aVR
But as a review summarized, “While all have proven their value in distinguishing VT and SWCT, no single criterion or collection of criteria promises diagnostic certainty.”[3] Fascicular VT, for example, originates and uses the ventricular conducting system, so can give a typical aberrant morphology and can be found in young patients without heart disease (idiopathic VT). In the unstable patient it’s a moot point because they require immediate electrical cardioversion. In the stable patient with regular monomorphic WCT, adenosine is included in the guidelines as a therapeutic test (but not a diagnostic test, as some VT respond to adenosine). But “when doubt exists, it is safest to assume that any wide-complex tachycardia is VT, particularly in patients with known cardiovascular disease” and treat accordingly: procainamide or electrical cardioversion.[4]
ST changes can be secondary to the tachycardia itself, secondary to abnormal conduction, a primary abnormality from ischemic, metabolic or toxic causes—or a combination. So analysis of the ST segment and T waves needs to be put in context of the rest of the ECG, and the patient.
Back to the cases
Case 1: sinus tachycardia from TCA-type OD
- Heart rate/rhythm: sinus tach (biphasic seen clearly in V1, and upright P superimposed on T wave in lead II)
- Electrical conduction: borderline QRS (100ms), long QT (580ms)
- Axis: incomplete RBBB, borderline right axis
- R-wave: delayed R wave progression, tall terminal R in aVR
- Tension: no hypertrophy
- ST/T: no changes
Impression: TCA-type OD (from benadryl OD): sinus tach, sodium channel blockade (borderline QRS, S wave in I, tall R wave in aVR) and prolonged QT. Treated with fluids, sodium bicarb and magnesium, with resolution of changes.

Case 2: SVT with rate-related ST changes
- H: regular NCT without preceding P waves = SVT (computer misread T waves for P waves but the rate is too fast for sinus tach: 220 – age 70 = 150)
- E: normal conduction
- A: normal axis
- R: normal R wave
- T: no hypertrophy
- S: diffuse STD and reciprocal STE in aVR
Impression: SVT with rate-related ST changes. Treated with modified Valsalva: NSR without ST changes

Case 3: rapid AF with rate-related ST changes
- H: irregularly irregular NCT without P waves = atrial fibrillation
- E: otherwise normal conduction
- A: old left axis
- R: old early R wave progression
- T: no hypertrophy
- S: diffuse STD with reciprocal STE in aVR
Impression: rapid Afib with rate-related changes. Cath lab activated due to”STE-avR STEMI-equivalent” but this in the context of rapid Afib. No obstructive lesions on cath, patient spontaneously converted to NSR and ST changes resolved:

Case 4: hyperkalemia
- H: regular wide complex rhythm without P wave = junctional escape (<120 so not fast enough for VT)
- E: nonspecific IVCD, LAFT
- A: extreme axis
- R: poor R wave progression
- T: no hypertrophy
- S: peaked T waves
Impression: multiple signs of hyperkalemia (potassium 8.6). Treated empirically with calcium, insulin/dextrose, fluids, ventolin. Repeat ECG had reappearance of P waves and narrow QRS, disappearance of LAFB, T waves still peaked:

Case 5: atrial fibrillation/flutter, and rate-related LBBB
- H: first ECG atrial fibrillation, second flutter waves with variable block
- E: first ECG narrow complex, second typical LBBB morphology
- A: normal axis
- R: delay R wave from LBBB
- T: no LVH in narrow complex rhythm
- S: rate-related inferolateral TWI in first ECG, proportional discordant ST/T changes in second ECG
Impression: rapid Afib/flutter with rate-related LBBB, in the context of dehydration. Treated first with fluids, and then rate control: resolved rate-related LBBB and rate-related ST changes

Case 6: polymorphic VT with normal QT, ischemia-related
Impression: polymorphic VT preceded by normal QT (i.e. not “torsades de pointes”). Treated with defibrillation and amiodarone. Post-ROSC ECG had anterior QS waves with T/QRS>0.36 suggesting recurring anterior occlusion MI, so taken back to cath lab: stent patent, and polymorphic VT attributed to recent myocardial ischemia.

Case 7: sinus tach with LBBB, with clinical and ECG signs of occlusion MI
- H: sinus tach (P waves visible V1-3)
- E: LBBB
- A: normal axis
- R: delayed R wave progression
- T: can’t assess LVH
- S: disproportionate STD in inferolaterally (STD>0.30 R wave), with disproportionate STE in aVR
Impression: LBBB with ischemic symptoms, unstable vitals and disproportionate ST changes, concerning for LBBB + Occlusion MI. After VF arrest taken to cath lab: triple vessel disease with 95% circumflex occlusion, peak trop 50,000
Case 8: sinus tach, RBBB+LAFB + Occlusion MI
- H: sinus tach (biphasic P in V1) with PACs
- E: LAFB and intermittent RBBB (eg V1-3 have RBBB on beats 2-3, conducting at same rate)
- A: left axis from LAFB
- R: anterior QS wave and QR wave during RBBB conduction
- T: no hypertrophy
- S: ST elevation anterolateral, toombstone morphology V3-6 exaggerating appearance of QRS, and inferior STD
Impression: chest pain with RBBB+LAFB+STE +tachycardia, concerning for left main or proximal LAD occlusion and hemodynamic compromise. Cath lab activated: 100% proximal LAD occlusion. First trop 85, peak 50k. Post-cath ECG: resolved RBBB, ongoing LAFB, persisting QS waves with STE (LV aneurysm morphology, wiht T/QRS<0.36):

Case 9: fascicular VT
- H: regular WCT without P waves = monomorphic VT >> SVT with abberancy
- E: typical RBBB + LAFB
- A: left axis from LAFB
- R: early R wave from RBBB
- T: no hypertrophy
- S: secondary ST/T changes
Impression: young patient with WCT with RBBB/LAFB morphology, typical of fascicular VT. Treated with cardioversion, with resolution of RBBB/LAFB. Follow up diagnosis of fascular VT

Case 10: monomorphic VT, scar-related
- H: regular WCT without P waves = monomorphic VT >> ST with abberancy
- E: LBBB morphology but slow r peak, long rS time, and slurred S wave
- A: left axis
- R: late R wave from LBBB
- T: can’t assess
- S: secondary ST/T changes
Impression: prior CAD with hemodynamically unstable WCT (and features of VT). Treated with electrical cardioversion, which restored NSR and revealed different baseline conduction (LBBB and left axis replaced by RBBB+LPFB with right axis). Symptoms resolved, vitals normalized, and admitted with negative workup. VT from old MI scar.

Take home points on ECG Cases 19 Tachycardias
- Search for sinus rhythm in leads V1 (biphasic P wave) and II (upright P wave)
- Consider reversible causes of WIDER supraventricular rhythms: WPW, IVCD (pre-existing or rate-related BBB), Drugs (sodium channel blockade), Electrolyte (hyperkalemia), Raised ST segment (STEMI)
- If the differential is monomorphic VT vs SVT with abberancy, assume VT
References for ECG Cases 19: Tachycardias
- Schlapfer J and Wellens H. Computer-interpreted electrocardiograms: benefits and limitations. J of Amer Coll Cardiol 2017 Aug 29;70(9): 1183-1192
- Hollowell H, Mattu A, Perron AD, et al. Wide-complex tachycardia: beyond the traditional differential diagnosis of ventricular tachycardia vs supraventricular tachycardia with aberrant conduction. Am J Emerg Med 2005 Nov;23(7):876-89
- Kashou AH, Noseworthy PA, DeSimone CV, et al. Wide complex tachycardia differentiation: a reappraisal of the state-of-the-art. J of Am Heart Assoc 2020 Jun 2;9(11):3016598
- Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS Guideline For The Management Of Adult Patients With Supraventricular Tachycardia: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2016;133:e506-e574



Leave A Comment