
Most Recent

BEEM Cases 3 – Acute Respiratory Failure: NIPPV & POCUS
Shortness of breath is a very common chief complaint in the emergency department, but despite our familiarity with this symptom, management is not always straightforward. The differential diagnosis is extensive, including the common cardiorespiratory conditions, but extending to toxicologic, hematologic, neuromuscular, metabolic, and psychiatric causes. Over the past decade, we have seen the widespread adoption of new technologies to help us manage these patients. This post will look at some new evidence on two of those technologies: noninvasive positive pressure ventilation (NIPPV) and ultrasound (POCUS). We will answer 3 questions based on 3 systematic reviews using the BEEM critical appraisal framework...
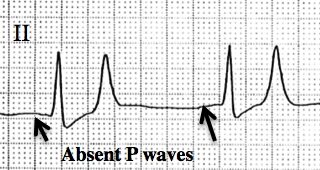
Best Case Ever 49 – Post-Arrest Hyperkalemia
Melanie Baimel's Best Case Ever on Post-Arrest Hyperkalemia on EM Cases. Post arrest patients can sometimes be challenging. We need to think of a variety of underlying causes of the arrest, antiarrhythmics, possible cath lab activation, targeted temperature management, sedation and more. To add to this, many post arrest patients do not have ideal vital signs that require attention. In this Best Case Ever, in anticipation of our upcoming episode on A Rational Approach to Hyperkalemia Dr. Melanie Baimel describes a post arrest patient who remains bradycardic and hypotensive despite multiple pressors....
Episode 85 – Medical Clearance of the Psychiatric Patient
Psychiatric chief complaints comprise about 6 or 7% of all ED visits, with the numbers of psychiatric patients we see increasing every year. The ED serves as both the lifeline and the gateway to psychiatric care for millions of patients suffering from acute behavioural or psychiatric emergencies. As ED docs, besides assessing the risk of suicide and homicide, one of the most important jobs we have is to determine whether the patient’s psychiatric or behavioral emergency is the result of an organic disease process, as opposed to a psychological one. There is no standard process for this. With the main objective in mind of picking up and appropriately managing organic disease while improving flow, decreasing cost and maintaining good relationships with our psychiatry colleagues, we have Dr. Howard Ovens, Dr. Brian Steinhart and Dr. Ian Dawe discuss this controversial topic...

CritCases 4 – Uterine Inversion and Postpartum Hemorrhage
In this CritCases blog - a collaboration between STARS Air Ambulance Service, Mike Betzner and EM Cases, Dr. James Brokenshire presents a case of acute unstable Uterine Inversion and discusses key therapeutic maneuvers including the Johnson Maneuver, tocolytics and resuscitation of postpartum hemorrhage.

Episode 84 – Congenital Heart Disease Emergencies
Congenital Heart Disease Emergencies on EM cases with Gary Joubert and Ashley Strobel. You might be surprised to learn that the prevalence of critical cardiac disease in infants is almost as high as the prevalence of infant sepsis. And if you’re like me, you don’t feel quite as confident managing sick infants with critical heart disease as you do managing sepsis. Critical congenital heart defects are often missed in the ED. For a variety of reasons, there are currently more children with congenital heart disease presenting to the ED than ever before and these numbers will continue to grow in the future. When I was in medical school I vaguely remember learning the complex physiology and long lists of congenital heart diseases, which I’ve now all but forgotten. What we really need to know about congenital heart disease emergencies is what actions to take in the ED when we have a cyanotic or shocky baby in front of us in the resuscitation room. So with the goal of learning a practical approach to congenital heart disease emergencies using the child’s age, colour and few simple tests, Dr. Strobel and Dr. Joubert will discuss some key actions, pearls and pitfalls so that the next time you’re faced with that crashing baby in the resuscitation room, you’ll know exactly what to do.

Journal Jam 7 – Amiodarone vs Lidocaine vs Placebo in Cardiac Arrest: The ALPS Trial
Journal Jam 7 - Amiodarone vs Lidocaine vs Placebo in Cardiac Arrest: The ALPS Trial. In our most popular EM Cases episode to date - ACLS Guidelines Cardiac Arrest Controversies, we boldly stated, that there has never been an antiarrhythmic medication that has shown any long term survival benefit in cardiac arrest. The use of medications in cardiac arrest has been one of those things that we all do, but that we know the evidence isn’t great for. Yet Amiodarone is still in the newest AHA adult cardiac arrest algorithm for ventricular fibrillation or pulseless ventricular tachycarida – 300mg IV after the 3rd shock with the option to give it again at 150mg after that. Anti-arrhythmics have been shown in previous RCTs to increase the rate of return of spontaneous circulation and even increased survival to hospital admission, however none of them have been able to show a decrease in mortality or a favourable neurological outcome at hospital discharge. In other words, there has never been shown a long term survival or functional benefit - which is a bit disconcerting. But now, we have a recent large randomized, controlled trial that shines some new light on the role of anti-arrythmics in cardiac arrest - The ALPS trial: Amiodarone vs Lidocaine vs placebo in out of hospital cardiac arrest. In this Journal Jam podcast, Justin Morgenstern and Anton Helman interview two authors of the ALPS trial, Dr. Laurie Morrison a world-renowned researcher in cardiac arrest and Dr. Paul Dorian, a cardiac electrophysiologist and one of Canada's leading authorities on arrhythmias about what we should take away from the ALPS trial. It turns out, it's not so simple. We also discuss the value of dual shock therapy for shock resistant ventricular fibrillation and the future of cardiac arrest care.
