
In this Part 1 of our two-part series on pericarditis and myocarditis, Anton is joined by Walter Himmel, EM doc at North York General and Paul Dorian cardiologist, researcher, and educator at St. Michael’s Hospital in Toronto (with a short visit from @ECG Cases Jesse McLaren). They answer questions such as: why should pericarditis be considered a diagnosis of exclusion? Which clinical features are most useful in the diagnosis of pericarditis? What are the most common pitfalls in the ECG interpretation of a patient suspected of pericarditis? What are the best ways to differentiate the ECG of pericarditis from that of MI and early repolarization? How is uncomplicated viral pericarditis treated differently compared to pericarditis of other etiologies? Why is it so important to include colchicine as part of the treatment of pericarditis? Which patients with pericarditis should be considered for admission? and many more…
Podcast: Play in new window | Download (Duration: 1:21:09 — 74.4MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman
Written Summary and blog post by Kate Dillon, edited by Anton Helman March, 2022
Cite this podcast as: Helman, A. Himmel, W. Dorian, P. Pericarditis and Cardiac Tamponade. Emergency Medicine Cases. March, 2022. https://emergencymedicinecases.com/pericarditis-cardiac-tamponade. Accessed [date]
Go to part 2 of this 2-part podcast on pericarditis and myocarditis
Pericarditis as a diagnosis of exclusion
Pericarditis should be considered a diagnosis of exclusion, after ruling out the big chest pain killers (MI, PE, aortic dissection, esophageal rupture, and tension pneumothorax), because it can be easily confused with these more time-sensitive, deadly diagnoses. Avoid premature closure!
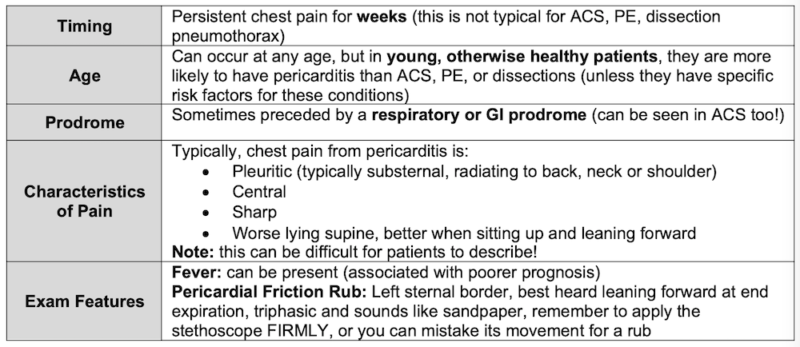
The following features are suggestive of pericarditis, but none alone have good enough test characteristics to rule it in or out.
Clinical features of pericarditis
Pericarditis diagnostic criteria and evaluation
The diagnosis of pericarditis requires 2/4 of the following criteria:
- Chest pain – typically sharp, pleuritic, positional (>80- 90% of cases)
- Pericardial rub on auscultation (<1/3rd of cases)
- New widespread ST elevation or PR depression on ECG (up to 60% of cases)
- New or worsening pericardial effusion (up to 60% of cases)
Additional supportive findings:
- Elevated inflammatory markers (CRP, ESR, WBC count)
- Evidence of pericardial inflammation on imaging (contrast CT, cardiac MR)
Diagnostic evaluation for pericarditis
- Auscultate for friction rub (excellent specificity/poor sensitivity)
- ECG (see below)
- Ultrasound (see below)
- CXR (enlarged cardiac silhouette if associated with large pericardial effusion)
- WBC + diff – if very elevated consider bacterial cause such as TB and/or alternate diagnosis such as endocarditis
- ESR/CRP – thought to be useful to support diagnosis, risk stratify, assess effectiveness of treatment (serial evaluations) and predict recurrence
- Creatinine to asses for uremia as a cause
- Troponin to help rule out ACS and myopericarditis
Pearl: CRP it thought to be helpful in pericarditis diagnosis, risk stratification, assessing effectiveness of treatment through serial evaluations and predicting recurrence
ECG in pericarditis – more than just diffuse ST elevation
The 4 stages of ECG changes in pericarditis
It is important to understand that the classic diffuse ST elevation/PR depression (stage 1) is only found in 60% of patients with pericarditis as patients may present to medical care at a more advanced stage. The temporal evolution of the 4 changes are highly variable and some patients may skip directly from stage 1 to stage 4 (normalization).
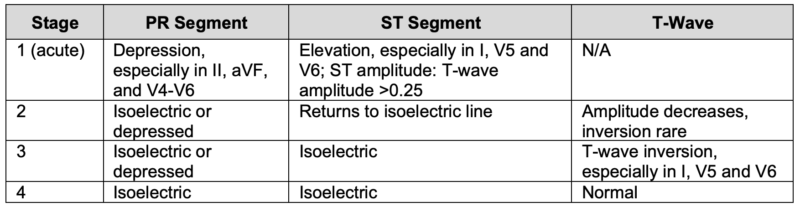

JACC VOL. 75, NO. 1, 2020 Chiabrando et al.
Pitfall: An important pitfall in ECG interpretation is failing to consider MI in a patient with chest pain and diffuse ST elevation on ECG; diffuse ST elevation can occur in MI.
Pitfall: Some patients evolve directly from Stage 1 to Stage 4 (normalization) before they present to ED, so the ECG may be normal with acute pericarditis. Do not rule out pericarditis based on a normal ECG.
Pearl: Uremic pericarditis does not cause significant inflammation of the epicardium, so the ECG and the inflammatory markers are more likely to be normal.
ECG findings to help differentiate Pericarditis from MI
No single ECG finding is diagnostic for pericarditis; all of the following findings can be seen in patients with cardiac ischemia, underlining the importance of approaching pericarditis as a diagnosis of exclusion.
- Widespread/diffuse PR depression and/or ST elevation
- J-point in pericarditis is usually sharper compared to a more blurred J point in MI
- ST elevations are more commonly convex shaped in STEMI, while concave upwards ST elevations are more typical of pericarditis
- If ST elevation or PR depression is present, there is typically a preservation of the normal upright T-waves in pericarditis (note however, that stage 3 is defined by T-wave inversions)
- ST elevation is rarely > 5mm in pericarditis
- ST depressions in V1 and aVR favor pericarditis
- aVL ST segment is typically elevated in pericarditis while aVL ST segment depression is highly specific for inferior MI
- Comparison of ST elevation in leads II and III may help differentiate STEMI from pericarditis
- ST elevation II > ST elevation III favors pericarditis
- ST elevation III > ST eleveation II is highly suspicious for inferior STEMI
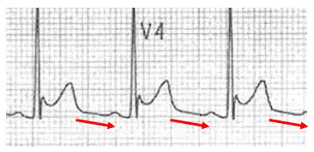
- Spodick’s sign is seen in approximately 80% of patients with acute pericarditis (and in 29% of patients with all stages of pericarditis) and 5% of STEMIs; it is characterized by down-sloping from the T wave to the QRS segments with the terminal PR segment depressed; this is best seen in lead II and the lateral precordial leads.
ECG findings of pericardial effusion that may be associated with pericarditis:
- Low voltages (also seen in COPD, and patients with obesity)
- Electrical alternans
Pitfall: There are no ECG findings that are 100% sensitive for specific to differentiate pericarditis from MI underlining the importance of approaching pericarditis as a diagnosis of exclusion
ECG findings to help differentiate pericarditis from early repolarization
Early repolarization is typically a phenomenon of young, healthy, tall athletes. This population overlaps with that of pericarditis.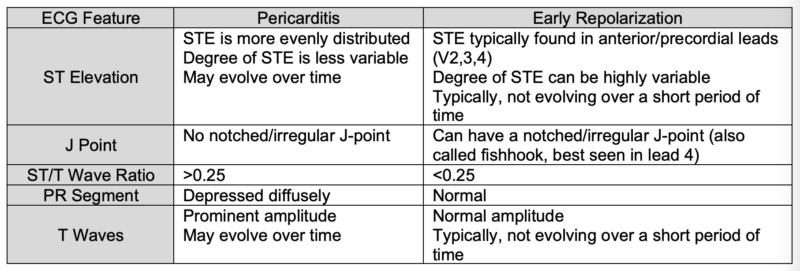
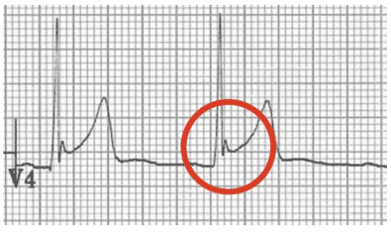
Example: Notched J-Point in early repolarization
PoCUS and pericarditis
Pericardial effusion found on PoCUS supports the diagnosis of pericarditis (60% of patients with pericarditis) but is not diagnostic.
The presence of a large pericardial effusion can help identify patients with acute pericarditis who are at higher risk for complications. If there are signs of LV dysfunction, consider myopericarditis.
To semi-quantitatively describe the size of a pericardial effusion, measure the echo-free space between the pericardial layers at end-diastole.
- Trivial: fluid is only seen in systole
- Small: <10 mm
- Moderate: 10-20 mm
- Large: 21-25mm
- Very Large: >25mm
The larger the pericardial effusion, the more likely cardiac tamponade is present; however, cardiac tamponade may occur with small-moderate pericardial effusions.
Troponin – the importance of trending troponins in suspected pericarditis
Troponin may be elevated in a number of chest pain presentations including pericarditis, myocarditis, pulmonary embolism and ACS. The troponin elevation in pericarditis typically remains stable over hours whereas the troponin elevation in MI typically increases over hours in the acute phase. Only a proportion of patients with pericarditis bump their troponin, and usually to a smaller degree compared to patients with myopericarditis and myocarditis.
Inflammatory markers – their utility in pericarditis
CRP elevation can be somewhat useful to support a diagnosis of pericarditis (a CRP >3 has a sensitivity of 80% for pericarditis). An elevated CRP also suggests a higher risk of recurrence and may be helpful serially to assess the clinical course. A very high CRP increases the likelihood of myopericarditis.
Differential diagnosis of pericarditis
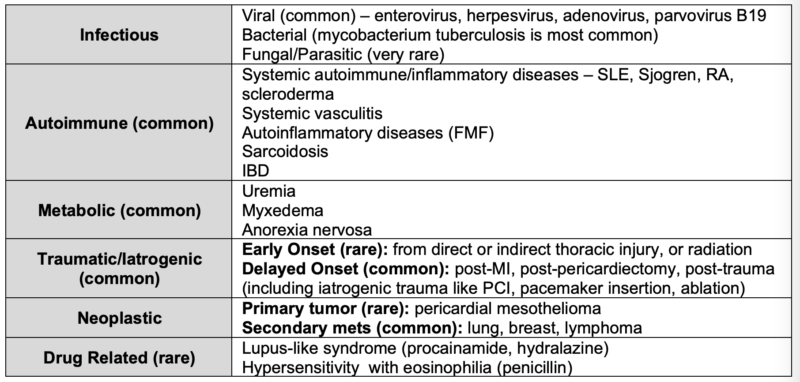
COVID associated pericarditis with be covered in Part 2 of this series.
Cardiac Tamponade – a rare life-threatening complication of pericarditis
Pericardial effusion and cardiac tamponade should be considered in all patients with pericarditis, especially those with a non-viral underlying etiology such as malignancy, TB or severe hypothyroidism.
Pearl: The presence of a large pericardial effusion and/or cardiac tamponade increases the likelihood of a non-viral cause of pericarditis and should trigger a search for a non-viral cause.
Cardiac tamponade is a clinical diagnosis, not an imaging one. While the larger the pericardial effusion, the more likely cardiac tamponade, it is not the size of the effusion alone that matters. Rather, it is the pressure on the right side of the heart that is the keystone of tamponade physiology. Small effusions that collect rapidly can lead to tamponade.
Pitfall: a common pitfall in the diagnosis of cardiac tamponade is ruling out tamponade just because the pericardial effusion is small
Clinical features of cardiac tamponade
5 features occur in the majority of patients with tamponade:
- Dyspnea (sensitivity 87-89%)
- Tachycardia (sensitivity, 77%)
- Pulsus paradoxus (with pericardial effusion) >10mmHg (sensitivity, 82%; LR+ 3.3), <10mm Hg (LR-0.03)
- Elevated JVP (sensitivity, 76%)
- Cardiomegaly on chest radiograph (sensitivity, 89%)
Pearl: When the decision to perform a pericardiocentesis needs to be made rapidly, a quick way to assess for pulsus paradoxus is to simply palpate the radial pulse for an inspiratory fall in BP rather than search for a sphygmomanometer (which are sometimes difficult to locate in the ED) and perform the more time-consuming traditional assessment for pulsus paradoxus
PoCUS findings suggestive of cardiac tamponade – scrutinize the right side of the heart and IVC
- A pericardial effusion >25mm (but smaller pericardial effusions can cause tamponade)
- Diastolic right ventricular collapse (high specificity)
- Systolic right atrial collapse (earliest sign)
- A plethoric inferior vena cava with minimal respiratory variation (high sensitivity)
- Exaggerated respiratory cycle changes in mitral and tricuspid valve in-flow velocities as a surrogate for pulsus paradoxus
Pearl: in patients with suspected cardiac tamponade where the diagnosis is not clear, consider a fluid bolus which may make the right heart PoCUS signs and pulsus paradoxus more obvious as well as increase filling pressure and cardiac output (avoid if severe, pre-existing LV dysfunction)
PoCUS Cases pericardial effusion- techniques and pitfalls
5 Minute Sono on pericardial tamponade
If the diagnosis of cardiac tamponade is unclear, consider:
- If the patient is clinically stable, a STAT echocardiogram done by an ultrasound tech
- Placing an arterial line for continuous monitoring for pulsus paradoxus
- Performing a pericardiocentesis which is both diagnostic and therapeutic
Pitfall: a common pitfall in the management of cardiac tamponade is delaying pericardiocentesis until the patient becomes hemodynamically unstable
Best Case Ever 31 on pericardiocentesis with Andrew Sloas
NEJM emergency pericardiocentesis
Treatment of pericarditis – don’t forget the colchicine!
The main goals of the treatment of pericarditis are
1. To reduce the acute inflammation with NSAIDs and
2. To prevent recurrence, constrictive pericarditis and long term morbidity with colchicine.
Be sure to include colchicine because it has been shown to prevent the most common complication of pericarditis – recurrent pericarditis (as apposed to NSAIDs which have not been shown to alter the natural history of acute pericarditis).
Outpatient management of pericarditis with a presumed idiopathic/viral cause
- Restrict strenuous physical activity which may trigger recurrence of symptoms
- Ibuprofen 600mg TID or indomethacin 50mg TID (for acute inflammation)
- Colchicine 0.6mg daily for <70kg, bid for ≥70kg (to help prevent recurrence)
- Evidence suggests reduction of recurrence rate by up to 50%
- May also facilitate rapid resolution of symptoms
- Warn patients of GI upset with colchicine
- PPI for those at high risk of UGIB (especially if using indomethacin, which has a high incidence of gastritis)
Duration of treatment with anti-inflammatories is based on resolution of symptoms and normalization of CRP (in uncomplicated cases, generally 1-2 weeks followed by taper). Colchicine treatment will sometimes continue for months. Ensure follow-up within a week and inform them that even if they start to feel better, they should continue medications until follow-up to prevent recurrence.
Corticosteroids – second line therapy; can lead to rebound pericarditis when it is stopped, and is associated with a higher risk for recurrent pericarditis
Treatment for patients with pericarditis due to non-viral causes:
- Cancer-related Pericarditis – many patients will have a large effusion requiring pericardiocentesis (or pericardial window if hemorrhagic effusion)
- Uremia-related Pericarditis – consider dialysis +/- pericardiocentesis; NSAIDs and colchicine are generally contraindicated in patients with pericarditis who have severe renal impairment
Treatment of patients with pericarditis who are taking anticoagulants/antiplatelet agents
These patients are at high risk for GI bleed if they require NSAIDs as well as hemorrhagic pericarditis requiring pericardial window; treatment decisions should be made in concert with cardiology/hematology.
Disposition for patients with pericarditis
- Patients who are otherwise healthy with uncomplicated presumed viral pericarditis, who have mild symptoms are generally safe to be discharged home with cardiology follow-up, medications, and instructions not to exercise (this is the majority of patients)
- Patients with pericarditis from a non-viral cause should be considered for admission and further workup of the etiology as these patients are more likely to develop complications and may require specific time-sensitive treatment
- Risk factors for poor prognosis which should prompt consideration for admission include:
- Fever (>38C)
- Failure to respond within 7 days to treatment
- Large pericardial effusion (>20mm)
- Oral anticoagulants
- Myocarditis (elevated troponin)
- Immunosuppression
Take Home Points for acute pericarditis
- Pericarditis is a diagnosis of exclusion after ruling out the big chest pain killers; avoid premature closure!
- No single clinical feature is diagnostic of pericarditis; symptoms over many days, young age, presence of a viral prodrome, sharp pleuritic positional chest pain, presence of a fever, a triphasic pericardial friction rub should all be considered contributory
- CRP may be helpful to risk stratify patients and predict recurrence; a troponin or serial troponins should be considered to help rule out ACS and myocarditis
- The main pitfall with ECG interpretation is failure to consider MI as a cause of diffuse ST elevation
- There are 4 stages of ECG changes in pericarditis, and the progression through these stages is variable; patients with pericarditis can have a normal ECG
- There are a number of features on ECG that can help to distinguish between MI and pericarditis and benign early repolarization, but no single feature is diagnostic
- Important pitfalls in the diagnosis and management of cardiac tamponade include delaying pericardiocentesis and assuming there is no tamponade when the size of the effusion is small or moderate
- In time-sensitive situations palpation (rather than using a BP cuff) for pulsus paradoxus is adequate for helping to make the diagnosis of cardiac tamponade rapidly
- Treatment of uncomplicated viral acute pericarditis includes NSAIDs as well as more prolonged treatment with colchicine to prevent recurrence
- Consideration should be given for gastric protection with a PPI for patients receiving high dose NSAIDS
- Patients with uncomplicated, viral pericarditis can usually be safely discharged home with appropriate follow-up, discharge instructions NSAIDs and colchicine; patients with an uncertain etiology or with risk factors for poor prognosis should be considered for admission for further work up and consideration for pericardial window, dialysis etc.
Go to part 2 of this 2-part podcast on pericarditis and myocarditis
References
- Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. European Heart Journal. 2015;36(42):2921-2964.
- Roy CL, Minor MA, Brookhart MA, Choudhry NK. Does This Patient With a Pericardial Effusion Have Cardiac Tamponade? JAMA. 2007;297(16):1810.
- Swaminathan A. REBEL Core Cast 68.0 – Pericarditis. Published online November 10, 2021. Accessed December 11, 2021. https://rebelem.com/rebel-core-cast-68-0- pericarditis/
- Imazio M, Gaita F, LeWinter M. Evaluation and Treatment of Pericarditis. JAMA. 2015;314(14):1498.
- DeYoung H, Sulava E. EM@3AM: Pericarditis. Published December 27, 2018. Accessed December 19, 2021. http://www.emdocs.net/em3am-pericarditis/
- Imazio M. Acute pericarditis: Clinical presentation, diagnostic evaluation, and diagnosis. UpToDate. Published April 16, 2021. Accessed December 21, 2021. https://www.uptodate.com/contents/acute-pericarditis-treatment-and-prognosis
- McLaren J. ECG Cases 27 Pericarditis – Diagnosis of Exclusion . Published online November 2021. Accessed December 11, 2021. https://emergencymedicinecases.com/ecg- cases-pericarditis-diagnosis-exclusion/
- Witting MD, Hu KM, Westreich AA, et al. Evaluation of Spodick’s sign and other electrocardiographic findings as indicators of STEMI and pericarditis. J of Emerg Med 2020;58(4):562-569.
- Bischof JE, Worrall C, Thompson P, et al. ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis. Am J of Emerg Med 2016;34:149-154.
- Bhardwaj R, Berzingi C, Miller C, et al. Differential diagnosis of acute pericarditis from normal variant early repolarization and left ventricular hypertrophy with early repolarization: an electrocardiographic study. Am J of Med Sci 2013 Jan;345(1): 28-32.
- Imazio M, Demichelis B, Cecchi E, et al. Cardiac troponin in acute pericarditis. Journal of the American College of Cardiology. 2003;42(12):2144-2148.
- Perera P, Mandavia D, Goodman A, Mailhot T. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade. Journal of Emergencies, Trauma, and Shock. 2012;5(1):72.
- Hoit B. Diagnosis and treatment of pericardial effusion. Published November 2021. https://www.uptodate.com/contents/diagnosis-and-treatment-of-pericardial- effusion#H4462972
- Farkas, J. EMCRIT. Pericardial Tamponade, November 10, 2021, https://emcrit.org/ibcc/tamponade/#rapid_reference
- Argulian E, Messerli F. Misconceptions and facts about pericardial effusion and tamponade. Am J Med. 2013 Oct;126(10):858-61.
- McCanny P, Colreavy F. Echocardiographic approach to cardiac tamponade in critically ill patients. J Crit Care. 2017 Jun;39:271-277.
- Kearns MJ, Walley KR. Tamponade: Hemodynamic and Echocardiographic Diagnosis. Chest. 2018 May;153(5):1266-1275.
- Honasoge AP, Dubbs SB. Rapid Fire: Pericardial Effusion and Tamponade. Emerg Med Clin North Am. 2018 Aug;36(3):557-565.
- Alerhand S, Carter JM. What echocardiographic findings suggest a pericardial effusion is causing tamponade? Am J Emerg Med. 2019 Feb;37(2):321-326.
- Chiabrando JG, Bonaventura A, Vecchié A, et al. Management of Acute and Recurrent Pericarditis. Journal of the American College of Cardiology. 2020;75(1):76-92.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine in Addition to Conventional Therapy for Acute Pericarditis. Circulation. 2005;112(13):2012-2016.
- Lotrionte M, Biondi-Zoccai G, Imazio M, et al. International collaborative systematic review of controlled clinical trials on pharmacologic treatments for acute pericarditis and its recurrences. American Heart Journal. 2010;160(4):662-670.
- Imazio M, Brucato A, Cemin R, et al. A Randomized Trial of Colchicine for Acute Pericarditis. New England Journal of Medicine. 2013;369(16):1522-1528.
- Alabed S, Cabello JB, Irving GJ, Qintar M, Burls A. Colchicine for pericarditis. Cochrane Database of Systematic Reviews. Published online August 28, 2014.
- Imazio M, Brucato A, Trinchero R, Spodick D, Adler Y. Individualized therapy for pericarditis. Expert Review of Cardiovascular Therapy. 2009;7(8):965-975.
- Hufnagel G, Pankuweit S, Richter A, Schonian U, Maisch B. The European Study of Epidemiology and Treatment of Cardiac Inflammatory Diseases (ESETCID). Herz. 2000;25(3):279-285.
- Imazio M, Cecchi E, Demichelis B, et al. Indicators of Poor Prognosis of Acute Pericarditis. Circulation. 2007;115(21):2739-2744.
Drs. Helman, Dorian and Himmel have no conflicts of interest to declare
Now test your knowledge with a quiz.



Leave A Comment