
In this ECG Cases blog we look at 9 pacemaker patients who presented to the emergency department, and provide a simple diagnostic approach using the PACER mnemonic that incorporates both the pacemaker and the patient.
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman, October 2022
9 pacemaker patients presented to the ED. What’s the diagnosis, and is it related to the pacemaker or the patient?
Case 1: 85 year old, history of MI, DDD pacemaker for AV block, with palpitations

Case 2: 80 year old, VVI pacer for AF with slow ventricular response, with shortness of breath, weakness and dizzy. HR 40, BP 160. Old then new:


Case 3: 85 year old, DDD pacemaker for sinus pauses, with pleuritic chest pain 5 days after pacemaker insertion

Case 4: 90 year old, history CAD and CHF with biventricular pacemaker, on spironolactone, with few days of weakness

Case 5: 75 year old, DDD pacemaker for hypertrophic cardiomyopathy, with an hour of chest pain and nausea

Case 6: 85 year old, history inferior MI, VVI pacemaker for AF with slow ventricular response, with acute chest pain

Case 7: 100 year old, history aortic stenosis and AF, VVI pacemaker for AV block, with generalized weakness, trop 300 ng/L

Case 8: 75 year old, DDD pacemaker for AV block, with weakness and confusion, HR 110 and BP 90. Old then new:


Case 9: 75 year old, history CAD, VVI pacemaker for AF, with few days weakness and presyncope. HR 60 BP 80

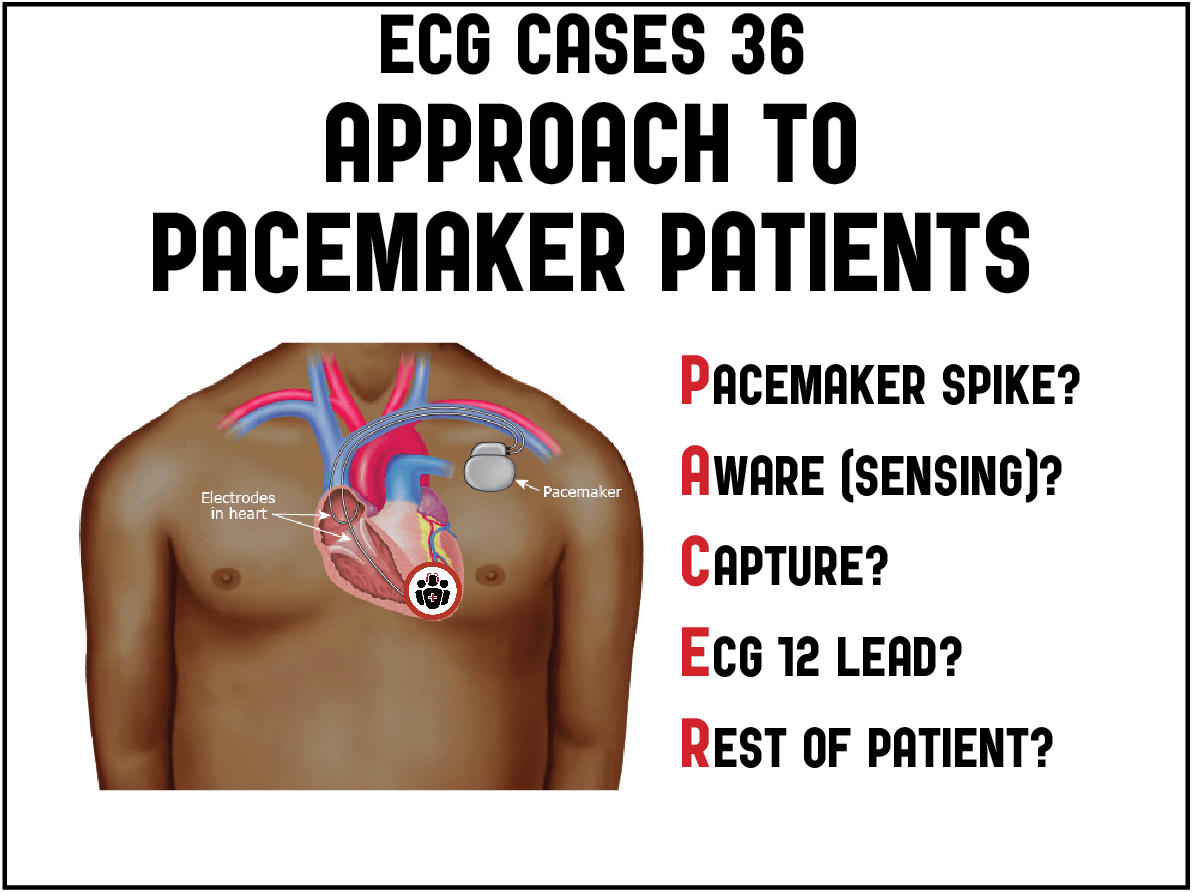
PACER mnemonic: ECG Approach to pacemaker patients
Common indications for permanent pacing include sinus node dysfunction causing symptomatic bradydysrhythmias, AV block, cardiac resynchronization for severe heart failure, or for termination of tachydysrhythmias. Atrial pacing in the right atrium produces a P wave similar to normal sinus rhythm, while right ventricular pacing mimics bundle branch block (usually LBBB, with a left axis and no R wave progression, from a pacemaker in the apex of the right ventricle).
Pacemakers are classified by a sequence of 3 letters specifying 1) the chamber(s) being paced (Atrial, Ventricular, or Dual), 2) the chamber(s) being sensed (Atria, Ventricular, Dual, or none), and 3) the response to sensing (Triggered, Inhibited, Dual, or none). For example, patients with sinus node dysfunction but normal conduction might only need their atria paced, and if intrinsic atrial activity is sensed the pacing is inhibited (AAI). In patients with AF and slow ventricular response, only the ventricle needs to be paced, and if ventricular activity is sensed the pacing is inhibited (VVI). Commonly patients get both right atrium and right ventricle paced and sensed, with the option of triggered activity (eg atrial activity triggers ventricular pacing) or inhibited activity (atrial activity inhibits atrial pacing, and ventricular pacing inhibits ventricular pacing) – in other words DDD. Patients with severe heart failure can get biventricular pacing for cardiac resynchronization. [1]
Pacemaker patients who present to the ED can have electrical or mechanical complications of the pacemaker [2,3], other medical emergencies visible on the paced ECG, or a normal pacemaker with an unrelated emergency. These can be assessed by a series of questions summarized by the mnemonic PACER, which starts by assessing pacemaker function on the rhythm strip (including pacing, sensing and capture), then looks at the rest of the 12 lead, and then looks at the rest of the patient:
PACER mnemonic for approach to pacemaker patients
Pacing spikes: are they present and appropriate?
- Normal pacing can include appropriate presence of spikes, or appropriate lack because of sensing intrinsic beats
- Pacemaker-mediated tachycardia: ventricular pacing triggers atrial pacing, leading to re-entry tachycardia, stopped by applying magnet to turn off sensing. Much more rare is runaway pacemaker, with extremely fast rates, treated by cutting the pacemaker wires
- Failure to pace: lack of appropriate pacing spikes. Applying a magnet turns off sensing, to differentiate over-sensing from batter depletion
Aware: is the pacemaker aware (sensing) intrinsic beats?
- Normal sensing: intrinsic beats are sensed and inhibit pacemaker
- Over-sensing (eg muscle contraction, or peaked T from hyperkalemia): results in underpacing, can be stopped by magnet
- Under-sensing (eg from lead migration, fibrosis, ischemia, hypekalemia): results in overpacing, with risk of R-on-T phenomenon and ventricular arrhythmia
Capture: if there are pacing spikes, do they trigger a beat?
- Normal capture: every pacing spike triggers a beat
- Failure to capture (eg ischemia, hyperkalemia, lead migration): pacing spike fails to trigger a beat
ECG: does the rest of the 12 lead ECG reveal any other problems?
- Hyperkalemia, can produce excessive conduction delay even for ventricular paced rhythms, which is important to identify and treat (especially since hyperkalemia can be a cause of pacemaker malfunction). As a review summarized, “pacemaker patients suspected of having hyperkalemia should be treated immediately without waiting for the result of the K level because their condition can deteriorate quickly.” [4]
- Occlusion MI (OMI) can be identified in ventricular paced rhythms: the Modified Sgarbossa Criteria, used to identify OMI in the presence of LBBB, has been validated in ventricular paced rhythms,[5] and inappropriately concordant ST elevation can identify LAD occlusion in the presence of RBBB. On the other hand, cardiac pacing can result in diffuse T wave inversion during intrinsic beats . These “memory T waves” point in the same direction as the paced QRS complexes, are deeper in the precordial than inferior leads, and are associated with upright T waves in I/aVL. [6]
Rest of the patient: are their complications from pacemaker insertion, or emergencies unrelated to the pacemaker?
- Pacemaker mechanical complications: these include complications related to the pocket (hematoma, infection), lead placement (pneumothorax, venous thrombosis, lead infection), or electrode-myocardium interface (lead migration, cardiac perforation). These can be identified by physical exam, POCUS or imaging
- Medical emergencies unrelated to pacemaker: patients with pacemakers are usually older and with comorbidities that are risk factor for other emergencies, eg dehydration, GI bleed, sepsis
Back to the cases for approach to pacemaker patients
Case 1: pacemaker electrical complication – failure to sense
- H: atrial flutter with variable block, intermittent inappropriate pacing (failure to sense), last spike happens during the T wave
- E: RBBB
- A: right axis
- R: early R wave from RBBB
- T: normal voltages
- S: secondary ST changes
Impression: failure to sense leading to inappropriate pacing. Developed R-on-T triggering ventricular arrhythmia, cardioverted.
Pacemaker fixed: ventricular pacing with appropriate sensing and capture

Case 2: pacemaker electrical complication – failure to capture.
- H: old ECG had left ventricular pacing, new ECG has RBBB escape rhythm with pacing and sensing but failure to capture
- E: RBBB morphology escape rhythm
- A: normal axis
- R: early R wave from RBBB
- T: normal voltages
- S: diffuse deep T wave inversions in same direction as prior paced QRS complexes, deeper precordial than inferior, and with upright T waves in I/aVL (cardiac memory)
Impression: failure to capture. Had normal labs, and pacemaker settings adjusted. Discharge ECG had normal ventricular pacing

Case 3: pacemaker mechanical complication – cardiac perforation
- Heart rate/rhythm: atrial paced with normal sensing and capture, followed by intrinsic ventricular beats which are all sensed (ventricular pacing inhibited)
- Electrical conduction: IVCD
- Axis: normal axis
- R-wave: delayed R wave progression
- Tall/small voltages: low voltages limb leads
- ST/T: secondary ST changes
Impression: normal pacemaker function, with pleuritic chest pain post-pacemaker insertion. POCUS showed pericardial effusion. Admitted to repair cardiac perforation.
Case 4: normal pacemaker but wide PR/QRS from hyperkalemia
- H: atrial and ventricular paced with appropriate sensing and capture
- E: prolonged PR, LBBB morphology with excessively prolonged QRS
- A: left axis
- R: delayed R wave progression
- T: normal voltages
- S: appropriate discordance
Impression: atrial/ventricular paced with prolonged PR/QRS in patient with weakness on spironolactone. Potassium 7.1. After calcium and reversal of hyperkalemia, QRS returned to normal width:

Case 5: normal pacemaker sensing bradycardia from infero-posterior STEMI(-)OMI
- H: all atrial paced with appropriate sensing and capture
- E: prolong PR, normal QRS/QT
- A: normal axis
- R: normal progression
- T: normal voltages
- S: inferior hyperacute T waves with reciprocal change in I/aVL, and anterior STD/TWI
Impression: atrial paced with infero-posterior STEMI(-)OMI.
Missed by physician. ECG repeated 2 hours later after troponin returned at 160 ng/L (normal <16 in females and <26 in males):

Now normal sinus rhythm (ie no longer bradycardic, so atrial pacing inhibited) with first degree AV block, more obvious infero-posterior OMI. Cath lab activated: 99% distal RCA occlusion (which can cause bradycardia). Peak troponin 45,000 ng/L and discharge ECG showed sinus rhythm with inferolateral reperfusion T wave inversion:

Case 6: normal pacemaker with concordant ST elevation from LAD occlusion
- H: ventricular paced with appropriate sensing and capture
- E: RBBB/LAFB with alternating morphology
- A: left axis
- R: early R wave
- T: normal voltages
- S: concordant ST elevation V2-4
Impression: LAD occlusion. Cath lab activated. ECG repeated prior to cath showed more dramatic precordial ST elevation

Cath: 100% distal LAD occlusion. First troponin 10ng/L (normal) and peak 300,000. Discharge ECG showed ventricular paced with reperfusion T wave inversion:

Case 7: normal pacemaker with appropriate discordance, patient had non-occlusive MI from demand ischemia
- H: ventricular pacing with appropriate sensing and capture
- E: LBBB morphology
- A: left axis
- R: no R wave progression as expected for LV apex pacing
- T: normal voltages
- S: appropriate discordance, including V2 where there is greater than 5mm ST elevation but this is appropriate for a QRS complex of 35mm (5/35 = 14%)
Impression: weakness and positive troponin, false positive by traditional Sgarbossa criteria but negative by modified Sgarbossa criteria. Troponin declined to 175, attributed to demand ischemia from aortic stenosis and dehydration from hypercalcemia
Case 8: normal pacemaker, patient tachycardic from sepsis
- H: sinus tachycardia with appropriate ventricular sensing + pacing + capture
- E: normal PR, wide QRS with LBBB morphology
- A: extreme axis from old left axis + RA/LA lead reversal
- R: delayed R wave progression as expected
- T: normal voltages
- S: appropriate discordance
Impression: sinus tachycardia with ventricular pacing, in patient with sepsis. Follow up ECG after treatment and correct lead placement returned to baseline:

Case 9: normal pacemaker but patient hypotensive from dehydration
- H: ventricular pacing with appropriate sensing (first beat intrinsic) and capture
- E: LBBB morphology
- A: left axis from paced rhythm
- R: delayed R wave progression
- T: normal voltages
- S: appropriate discordant ST changes
Impression: normal pacemaker but patient hypotensive. Treated with fluids and BP improved. Diagnosed with dehydration and COVID.
Take home points for PACER mnemonic approach to pacemaker patients
Pacemaker spike: is it appropriately presence/absent, is there pacemaker-mediated tachycardia (apply magnet) or is there failure to pace (apply magnet to stop sensing, cardio consult)?
Aware (sensing): is it normal, is there oversensing (underpacing: apply magnet) or undersensing (treat reversible causes, cardio consult)
Capture: if there are pacemaker spikes is there capture, or failure to capture (treat reversible causes, cardio consult)
ECG 12 lead: are there signs of hyperkalemia (extra wide QRS, peaked T) or Occlusion MI (Modified Sgarbossa Criteria) that need immediate treatment
Rest of patient: is there a complication of pacemaker insertion related to the pocket (hematoma, infection), lead (pneumothorax, DVT), or heart (pericardial perforation), or is there an emergency unrelated to the pacemaker (eg dehydration, sepsis, GI bleed)
Dr. Tarlan Hedayati will be speaking on pacemaker malfunction at EM Cases Summit 2023
References for ECG Cases 36 – PACER mnemonic approach to pacemaker patients
- Glikson M, Nilsen JC, Kronbord MB, et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) with the special contribution of the European Heart Rhythm Association (EHRA). Eur Heart J Sept 2021;42(35):3427-3520
- Cardall TY, Chan TC, Brady WJ, et al. Permanent cardiac pacemakers: issues relevant to the emerg physician, part I. J of Emerg Med 1999;17(3):479-489
- Cardall TY, Brady WJ, Chan TC et al. Permanent cardiac pacemakers: issues relevant to the emerg physician, part II. J of Emerg Med 1999;17(4):697-709
- Barold SS, Herweg B. The effect of hyperkalemia on cardiac rhythm devices. Europace 2014;16:467-476
- Dodd KW, Zvosec DL, Hart MA, et al. Electrocardiographic diagnosis of acute coronary occlusion myocardial infarction in ventricular paced rhythm using the Modified Sgarbossa Criteria. Ann Emerg Med 2021 Oct;78(4):517-529
- Gunaseelan R, Sasikumar M, Aswin K, et al. Memory T-waves, a rare cause of T-wave inversion in the emergency department. J Emerg Trauma Shock 2020 Oct-Dec;13(4):312-316



Leave A Comment