
Topics in this EM Quick Hits podcast
Salim Rezaie on HALT-IT trial for TXA in unstable GI bleed (0:30)
Sarah Reid on pediatric DKA update in fluid management and cerebral edema (8:32)
Hans Rosenberg on POCUS in shoulder dislocations via CJEM (15:30)
Arun Sayal on Lisfranc injury pearls and pitfalls (23:57)
Justin Morgenstern on RECOVERY Trial for Dexamethasone in COVID pneumonia (32:48)
Walter Himmel on getting what you need from consultants (38:41)
Podcast: Play in new window | Download (Duration: 52:20 — 48.0MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content by Salim Rezaie, Sarah Reid, Hans Rosenberg, Tara Dahn, Arun Sayal, Justin Morgenstern, Walter Himmel and Anton Helman
Written summary & blog post by Graham Mazereeuw, edited by Anton Helman
Cite this podcast as: Helman, A. Rezaie, S. Reid, S. Rosenberg, H. Dahn, T. Sayal, A. Morgenstern, J. Himmel, W. EM Quick Hits 21 – The HALT-IT Trial for TXA in Unstable GI Bleed, Pediatric DKA Update in Fluid Management and Cerebral Edema, POCUS in Shoulder Dislocations, Lisfranc Injury Pearls and Pitfalls, the RECOVERY Trial for Dexamethasone in COVID Pneumonia, Consulting Tips. Emergency Medicine Cases. August, 2020. https://emergencymedicinecases.com/em-quick-hits-august-2020/. Accessed [date].
HALT-IT Trial for TXA in Unstable GI Bleed
- Largest trial yet: international, multicenter RCT, 12,000 adults with significant GI bleeding (90% upper GI bleed)
- Intervention: TXA 1g IV infusion followed by 3g maintenance infusion over 24 hours vs. placebo
- No difference in 5-day mortality due to bleeding between TXA (4%) and placebo (4%) (risk ratio 0.99, 95% CI 0.82 to 1.18)
- TXA did not reduce the need for transfusion or surgical intervention; no benefit from early administration (< 3 hours)
- Small, but significant increase in VTE risk with TXA (NNH=250)
Bottom line: TXA should not be routinely recommended for management of acute GI bleeds
Episode 101 GI Bleed Emergencies Part 1
- HALT-IT Trial Collaborators. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial. Lancet. 2020;395(10241):1927-1936.
- Bennett C, Klingenberg SL, Langholz E, Gluud LL. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2014;(11):CD006640.
- Chauncey JM, Wieters JS. Tranexamic Acid. [Updated 2019 Dec 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532909/
Pediatric DKA Update on Fluid Management and Cerebral Edema
- A practice changing PECARN study compared two fluid protocols in 1,389 cases of DKA
- Fast protocol: 10 mL/kg bolus + 10 mL/kg bolus (both with NS) followed by replacement of a 10% fluid deficit + maintenance over 36 hours with either NS or 0.45 NS
- Slow protocol: 10 mL/kg bolus (with NS) followed by replacement of a 5% fluid deficit + maintenance over 48 hours with either NS or 0.45 NS
- No difference between the fluid protocols in worsening mental status, cerebral injury, or post-DKA cognitive function
Bottom line: we don’t have to be so judicious with fluids in pediatric DKA; it’s almost always safe to start your resuscitation with 10mL/kg NS bolus regardless of fluid status and repeat if still hypoperfused

pediatric DKA algorithm
- Kuppermann N, Ghetti S, Schunk JE, et al. Clinical Trial of Fluid Infusion Rates for Pediatric Diabetic Ketoacidosis. N Engl J Med. 2018;378(24):2275-2287.
- Wolfsdorf JI, Glaser N, Agus M, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Pediatr Diabetes. 2018;19 Suppl 27:155-177.
- TREKK DKA Bottom Line Recommendations: https://trekk.ca/system/assets/assets/attachments/402/original/2019-06-18_DKA_BLR_v_3.1.pdf?1561062009 (accessed Jan 14, 2020)
- TREKK DKA Development Team: https://trekk.ca/system/assets/assets/attachments/350/original/2019-01-11_DKA_Refs_and_Devt_Team.pdf?1547230365 (accessed Jan 14, 2020)
POCUS for Shoulder Dislocations – CJEM ‘Just the Facts’
- Up to 70% of posterior shoulder dislocations may be missed on initial exam
- Posterior dislocations are uncommon and present less obviously compared to anterior shoulder dislocations (no shoulder squaring)
- Standard x-ray views usually have subtle findings and the axillary view x-rays, which are very helpful to detect a posterior shoulder dislocation, are often difficult to obtain as pain may impede the necessary shoulder positioning; CT scans are not always available as a backup
- Missed posterior dislocation can delay diagnosis and predispose patients to the need for surgical reduction
- Shoulder POCUS
- Posterior approach, transverse orientation, at the lateral edge of scapular spine
- Linear probe (ideal for thin patients) or curvilinear probe (ideal for larger or muscular patients)
- Sensitivity 99.1-100%, specificity 99.9-100% for dislocation
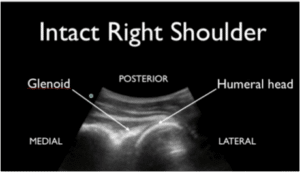
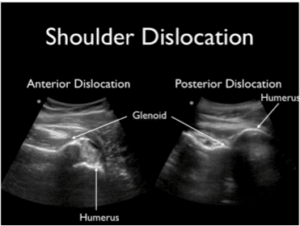
Figure 2. Shoulder POCUS with normal appearance (above) and dislocations (below) anteriorly and posteriorly
Bottom line: there might be a role for POCUS in the diagnosis and reduction of posterior shoulder dislocation; but usually the reason we miss this diagnosis is a lack of thorough history and physical (see EM Cases podcast on shoulder injuries ); a block to external rotation of the shoulder is highly suggestive of posterior shoulder dislocation.
Ep 135 Commonly Missed or Mismanaged Shoulder Injuries – Approach and Glenohumeral Dislocations
Ep 136 Occult Shoulder Injuries and Proximal Humerus Fractures
- Henneberry R, Dahn T, Atkinson P. Just the Facts: Point-of-care ultrasound in the management of shoulder dislocations. CJEM. 2020;22(3):287-290.
- Boswell B, Farrow R, Rosselli M, et al. Emergency Medicine Resident-Driven Point of Care Ultrasound for Suspected Shoulder Dislocation. South Med J. 2019;112(12):605-609.
- Gottlieb M, Holladay D, Peksa GD. Point-of-care ultrasound for the diagnosis of shoulder dislocation: A systematic review and meta-analysis. Am J Emerg Med. 2019;37(4):757-761.
- EMC Ep 135, Commonly missed or mismanaged shoulder injuries – Approach and glenohumeral dislocations https://emergencymedicinecases.com/shoulder-injuries-glenohumeral-dislocations/
Lisfranc Injuries Pearls and Pitfalls
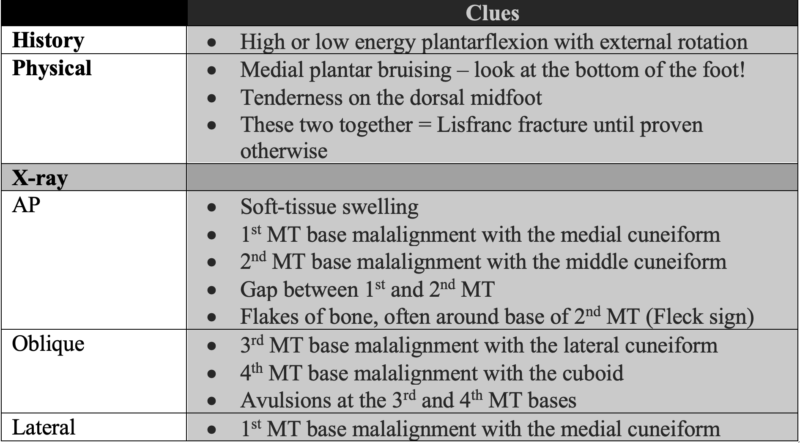

Fleck sign for avulsion fracture in Lisfranc injury
- History and physical exam are keys to this diagnosis
- Scrutinize x-rays with a keen eye, but avoid reliance on imaging; some Lisfranc injuries are radio-occult
- Displaced injury = unstable = operative management; undisplaced Lisfranc injuries – including ligamentous injuries – can also be unstable, so speak to your orthopaedic surgeon to help guide management
For more on Lisfranc injuries: EM Cases Digest, Volume 1: MSK & Trauma
Ep 178 Hand Injuries – Pitfalls in Assessment and Management
- EM Cases Digest, Volume 1: MSK & Trauma. https://emergencymedicinecases.com/wp-content/uploads/2015/05/EM-Cases-Digest-Vol-1-MSK-and-Trauma.pdf
- Blomberg, J. Lisfranc Injuries. OrthoBullets. July 2020: https://www.orthobullets.com/foot-and-ankle/7030/lisfranc-injury
RECOVERY Trial for Dexamethasone in COVID Pneumonia
- Design: 6,425 hospitalized patients with suspected or confirmed COVID-19 pneumonia in 176 hospitals in the United Kingdom; 2,104 patients randomized to dexamethasone with 4,321 controls
- Intervention: dexamethasone 6 mg daily PO or IV vs. usual care (unblinded)
- Dexamethasone might save lives! All-cause mortality was lower among patients treated with dexamethasone (21.6%) compared to controls (24.6%) (RR 0.65, 95% CI 0.51 to 0.82, NNT=33)
- Greatest benefits of dexamethasone were in ventilated patients > oxygenated patients > patients on room air
Bottom line: for patients with presumed COVID-19 pneumonia requiring ventilation or oxygen, even with an oxygen saturation of 92 to 94%, dexamethasone is probably your best bet for medical treatment
- Horby P, Lim WS, Emberson JR, et al. Dexamethasone in Hospitalized Patients with Covid-19 – Preliminary Report. N Engl J Med. 2020; Jul 17. doi: 10.1056/NEJMoa2021436.Online ahead of print.
- Johnson DB, Lopez MJ, Kelley B. Dexamethasone. [Updated 2020 Apr 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482130/
None of the authors have any conflicts of interest to declare



Leave A Comment