
Cardiovascular
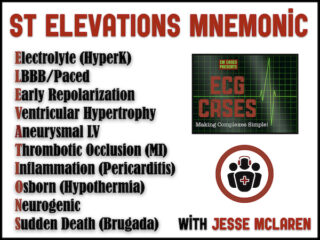
ECG Cases 17 – ST ELEVATIONS mnemonic and Occlusion MI
In this ECG Cases blog we look at 10 patients who presented with ST elevation, and review the differential diagnosis of ST elevation using the ELEVATIONS mnemonic. Which had occlusion MI?
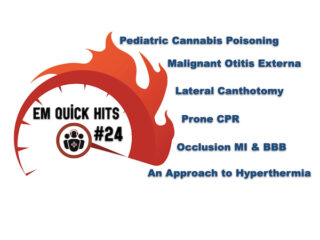
EM Quick Hits 24 Lateral Canthotomy, Cannabis Poisoning, Hyperthermia, Malignant Otitis Externa, BBB in Occlusion MI, Prone CPR
In this month's EM Quick Hits podcast: Anand Swaminathan on lateral canthotomy, Emily Austin on pediatric cannabis poisoning, Reuben Strayer on an approach to hyperthermia, Brit Long on diagnosis and management of malignant otitis externa, Jesse McLaren on ECG diagnosis of occlusion MI in patients with BBB and Peter Brindley on prone CPR...
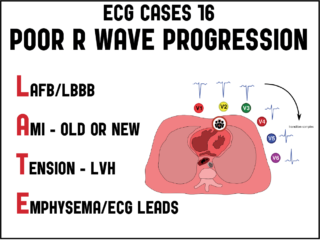
ECG Cases 16: Poor R-wave progression – The LATE mnemonic
In this ECG Cases blog we examine 6 patients who presented with poor R wave progression, and the LATE mnemonic for the differential...
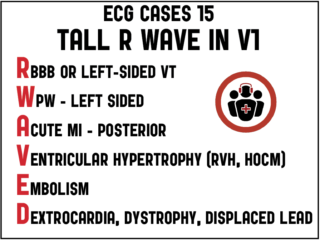
ECG Cases 15: Tall R Wave in V1
8 patients presented with ECGs showing a tall R wave in V1. What was the diagnosis? Jesse MacLaren reviews ECG interpretation of a tall R wave in V1 in this month's ECG Cases...
ECG Cases 14: Q-wave and Occlusion MI
9 patients presented with potentially ischemic symptoms and Q-waves. Which had Occlusion MI? What is the differential diagnosis of Q-waves? How can one distinguish MI vs LV aneurysm on ECG?...
ECG Cases 13: LVH and Occlusion MI
LVH produces secondary repolarization abnormalities that can mimic STEMI. Signs of occlusion MI in patients with LVH include: new Q waves/loss of R waves, disproportionate and dynamic ST elevation (or ST depression from posterior MI), and hyperacute T waves. In this ECG Cases blog we look at 6 patients who presented with potentially ischemic symptoms and LVH on their ECG. Which had an acute coronary occlusion?
