

This is EM Cases Episode 110 – Airway Pitfalls Live from EMU 2018.
The last decade has seen a torrent of literature and expert opinion on emergency airway management. It is challenging to integrate all this new information into a seamless flow when faced with a challenging airway situation. In this live podcast recorded at North York General’s Emergency Medicine Update Conference 2018, Scott Weingart and Anton Helman put together the latest in emergency airway management by outlining 6 common airway pitfalls: Failure to prepare for failure, failure to position the patient properly, failure to optimize oxygenation, failure to optimize hemodynamics, failure to consider an awake intubation and failure to prepare for a cricothyrotomy…
Podcast: Play in new window | Download (Duration: 40:09 — 36.9MB)
Subscribe: Apple Podcasts
Podcast production, sound design & editing by Anton Helman
Written Summary and blog post Anton Helman May, 2018
Cite this podcast as: Weingart, S, Helman, A. Airway Pitfalls – Live from EMU 2018. Emergency Medicine Cases. May, 2018. https://emergencymedicinecases.com/airway-pitfalls-emu/. Accessed [date].
First, slow down. In the vast majority of airway management situations, you have time. Rushing towards endotracheal intubation without adequate preparation is a recipe for disaster.
Beat The Stress Fool is a just-in-time stress management technique. It allows you to control your own physiology (heart rate, respiratory rate, stress response) when you anticipate a stressful situation. There are 4 techniques that you can choose one or more to do when a stressful situation arises.

Adapted from Mike Lauria, Annals of EM 2017
Breath – tactical breathing – slow down your breathing by counting 4 seconds while you inhale, hold your breath, then count to 4 secs while you exhale, then hold your breath (“box breathing“).
Talk – self talk – speak to yourself using positive cues such as “I got this”.
See – visualize yourself doing the procedure or actions perfectly which augments your chances of success.
Focus – use a trigger word such as “smooth” to slow and calm yourself down and focus on the task at hand.
EMCrit podcast on Beat The Stress Fool
Airway Pitfall #1: Failure to prepare for failure
ABC plans: Have a plan A, plan B if plan A fails and plan C if plan B fails.
Plan A is primary laryngoscopy – either VL or DL. A recent RCT suggests using VL with a Bougie to optimize first attempt success in anticipated difficult airways. After 3 attempts with a change in VL vs DL, position and/or intubators, move on to plan B.
Plan B is rescue with a supraglottic device (e.g. i-gel, LMA, AirQ, King LT). If the supraglottic device does not result in rapid improvement in oxygenation and end tidal CO2, declare to your team that you are in a “can’t intubate, can’t oxygenate” situation and move on to plan C – cricothyrotomy.
LMA description, insertion, contraindications and complications on LiTFL
Minimal failed airway bedside gear list within arms reach:
For plan A: VL, DL, ETT, Bougie, end tidal CO2
For plan B: supraglottic airway device
For plan C: scalpel, Bougie, size 6 ETT
Complete intubation checklist from EMCrit

Simplified cric kit to have prepared at the bedside
Verbalize your plan A, B and C to your team
For example: “I’m gonna take the first attempt at laryngoscopy with VL and bougie and if that fails I’m gonna try DL. If those two fail, Dr. Smith, the most experienced intubator in the room, is gonna take over. If our 3 attempts fail, we’ll place a supraglottic device, and if we can’t get a good pulse oxygenation and end-tidal CO2 witht the supraglottic device, we’re going to cut the neck.”
In this way, you’ve empowered your team to anticipate every move and to remind you if you go off plan.
Prepare your pressors
Consider hanging a norepinephrine drip running at 10 micrograms/min in a large antecubital peripheral line before securing the airway in all septic patients and all patients who you anticipate might drop their BP as a result of endothracheal intubation.
In addition, have “push-dose” epinephrine 10 micgrograms/mL mixed, drawn up and labeled with the concentration in the event that the BP tanks during or after intubation.
Aim for a MAP of 80 or SBP of 120-140.
Consider marking the cricothyroid membrane in advance of laryngoscopy.
Palpating for the cricothyroid membrane and marking it with an indelible marker in advance, not only allows faster access to the anatomy during surgical cricothyrotomy but mentally prepares you and your team to pull the trigger on going ahead with the procedure as soon as it becomes necessary. The greatest barrier to performing a cricothyrotomy isn’t the difficulty of the procedure itself, but rather, mentally acknowledging that a cric is what needs to be done now.
For more on preparation for airway management and the PREPARE mnemonic go to Peter Brindley’s Best Case Ever
Airway Pitfall #2 Failure to Position the Patient Properly
Maintain the patient in an upright position for as long as possible prior to laying them to 20-30 degrees in order to minimize lung atelectasis and decrease work of breathing.
There are 3 elements of patient position to optimize endotracheal intubation:
- Ear to sternal notch – a line drawn from the external meatus of the ear to the sternum should be parallel with the ceiling
- Face parallel to ceiling – bring the jaw up so that the face is parallel to the ceiling
- Base of neck flexion – ensure that the base of the neck is slightly flexed

Care of Nicholas Chrimes
The head rotation trick for easier BVM ventilation
If you are having difficulty bagging the patient after they have been paralyzed or maintaining oxygenation and adequate end tidal CO2, besides using an oral airway and a proper two handed BVM technique, one trick is to rotate the patient’s neck about 45 degrees. This may overcome the resistance you were feeling with BVM ventilations. If this doesn’t improve things go immediately to Plan B – supraglottic device.

From Cliff Reid’s Resus.me
Cliff Reid’s post on head rotation for mask ventilation
The head lift maneuver to bring the cords into view
After you’ve positioned the patient properly as described above and you still can’t achieve a good view of the cords, consider a head lift maneuver as shown in this video care of George Kovacs and the AIME Course.
Avoid over-leavering video laryngoscope
As shown in this video and in a recent RCT, a deliberately restricted laryngeal view with the GlideScope® video laryngoscope is associated with faster and easier tracheal intubation when compared with a full glottic view. If you over-leaver the video laryngoscope it can make it difficult to place the endotracheal tube through the cords. If this happens consider pulling back a bit on the scope to give you a partial view, which may allow easier passage of a Bougie or endotracheal tube. Video care of Dr. Max Ben Yakov and Hospital for Sick Children ED Group
Airway Pitfall #3: Failure to Optimize Oxygenation
As described in EM Cases Episode 54 – Preoxygenation and Delayed Sequence Intubation, the “triple 15 rule” can help to optimize oxygenation and denitrogenation prior to intubation which may protect patients from life-threatening desaturation during endotracheal intubation. Apply at least 15L O2 via nasal prongs, plus at least 15L O2 via non-rebreather, and if oxygen saturation <95-100% then apply 15cm H2O of CPAP while maintaining nasal prongs either via bag-valve-mask with a PEEP valve, using a good mask seal over nasal prongs, or by placing the patient on CPAP, also leaving the nasal prongs on. Use up to a maximum of 15cm H2O to prevent opening the lower esophageal sphincter.

Airway Pitfall #4: Failure to Optimize Hemodynamics for RSI
Aim for a SBP = 120-140 or a MAP = 80 prior to intubation.
This can be achieved during the 3 stages of airway management:
- Resuscitate before you intubate – consider crystalloid with the addition of norepinephrine infusion or blood products via a large antecubital peripheral IV or rapid transfuser depending on the particular clinical scenario.
- Induction and paralysis – for the hemodynamically precarious patient consider decreasing the sedation agent dose and increasing the paralytic agent dose to avoid a precipitous drop in BP during intubation. For example Ketamine 0.5mg/kg or 25-50mg IV in adults until the patient is dissociated and then Rocuronium 2mg/kg or 150-200mg IV in adults. Standard RSI doses of Ketamine (1-2mg/kg IV) may cause a precipitous drop in BP in those patients who are “catecholamine deplete”, and standard doses of Rocuronium (1mg/kg) in a patient in a shock state or poor cardiac output the onset of effect may take up to 4-5 minutes.
- After intubation – if the BP drops after intubation, consider the use of push dose pressors such as epinephrine drawn up prior to intubation as per this dosing.
Simplified dosing of sedation and paralytic agents in the hemodynamically compromised adult patient: Ketamine 50mg + Rocuronium 150mg
Airway Pitfall #5: Failure to Consider Awake Intubation
When to consider awake intubation
- Anticipated difficultly with ventilation (high BMI, significant facial trauma, Mallampati 4)
- Hemodynamic instability that persists despite usual pre-intubation resuscitation measures
- Poor oxygenation that persists despite employing the Triple 15 rule
- Altered airway anatomy (facial smash, epiglottitis)
- History of difficult/failed intubation
How to anesthetize for awake intubation (“topicalization”) by George Kovacs video #1

Care of Dr. Salim Rezaie, REBEL EM
Richard Levitan discussed airway management of morbidly obese ED patients in Episode 69
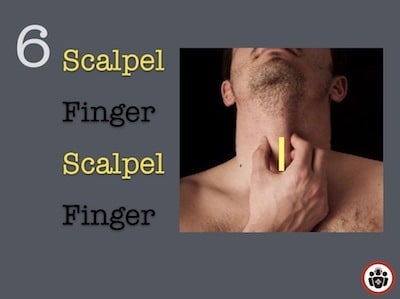
Airway Pitfall #6: Failure to Prepare for Cricothyrotomy
Surgical cricothyrotomy is indicated in “can’t intubate, can’t oxygenate scenarios”. This typically occurs after 3 failed DL and/or VL attempts followed by a failure to oxygenate adequately using a supraglottic device (Plan A, Plan B failure).
The procedure itself is not difficult. What is difficult (if you don’t prepare adequately) is the mental leap required to start doing the procedure. This psychological barrier can be overcome more easily if you prepare as outlined below.
The Difficult Airway Society guidelines recommend the scalpel-bougie technique.
Phase 1: Before you start your ED shift
- Familiarize yourself with a standardized challenging airway cart containing simple Bougie-assisted cric kit (Bougie, #10 scalpel, 6.0mm ETT).
- Establish a cohesive “difficult airway” program in your hospital based on current guidelines adapted to your specific environment.
- Two-step simulation training: low fidelity deliberate practice with simulation model followed by case-based simulation to augment psychological skills in a stressful situation.
- Post a standardized algorithm on the wall of your ED resuscitation room.
Details on Laura Duggan’s wearable cricothyrotomy trainer
Detailed anatomy on how to identify the cricothyroid membrane by Andy Neill
Phase 2: Before you perform the cric
- Mark the cricothyroid membrane with an indelible marker before any intubation attempt in anticipated challenging airway scenarios. This provides you and your team confidence in starting the procedure if it becomes necessary. Consider POCUS to aid in locating the cricothyroid membrane.
- Verbalize a failed airway plan and assign roles to your team.
- Clearly announce a “can’t intubate, can’t ventilate” situation.
Scalpel-Finger-Bougie technique details on Best Case Ever 71
A simple memory aid for performing a Bougie cricothyrotomy
General Airway poster for your ED by Dr. Caroline Shooner
Practice your cricothyrotomy skills with SimKit’s home delivery of their excellent cric model and simulation videos
Take Home Messages from Airway Pitfalls Live from EMU 2018
![]()
For more on airway management on EM Cases:
Airway Management Pocketbook – Rural
Episode 8: Emergency Airway Controversies
Episode 54: Preoxygenation and Delayed Sequence Intubation
Best Case Ever 39 – Airway Strategy & Mental Preparedness in EM Procedures
Best Case Ever 57 PREPARE mnemonic for Airway Management
Best Case Ever 62 Penetrating Upper Airway Injury Awake Intubation Do’s & Don’ts
CritCases 6 – Airway Obstruction
References
Guidelines for the management of tracheal intubation in critically ill adults. A Higgs B. British Journal of Anaesthesia. 2017
Lauria MJ, Gallo IA, Rush S, Brooks J, Spiegel R, Weingart SD. Psychological Skills to Improve Emergency Care Providers’ Performance Under Stress. Ann Emerg Med. 2017(6);884-890.
Gu Y, Robert J, Kovacs G, et al. A deliberately restricted laryngeal view with the GlideScope® video laryngoscope is associated with faster and easier tracheal intubation when compared with a full glottic view: a randomized clinical trial. Can J Anaesth. 2016;63(8):928-37.
Weingart, SD & Levitan, RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med, 2012;59(3): 165-75.
Ramachandran, SK, Cosnowski, A, Shanks, A & Turner, CR. 2010. Apneic oxygenation during prolonged laryngoscopy in obese patients: A randomized, controlled trial of nasal oxygen administration. J Clin Anesth, 22(3): 164-8.
Miller M, Kruit N, Heldreich C, et al. Hemodynamic Response After Rapid Sequence Induction With Ketamine in Out-of-Hospital Patients at Risk of Shock as Defined by the Shock Index. Ann Emerg Med. 2016;68(2):181-188.e2.
Driver, B, Prekker M. et al. Effect of Use of a Bougie vs Endotracheal Tube and Stylet on First-Attempt Intubation Success Among Patients With Difficult Airways Undergoing Emergency Intubation: A Randomized Clinical Trial.
Jaber S, Jung B, Corne P, et al. An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive care medicine. 2010; 36(2):248-55.
Frost PJ, Hingston CD, Wise MP. Reducing complications related to endotracheal intubation in critically ill patients. Intensive Care Med. 2010;36(8):1438.
Scott Weingart. Emergency Awake Topicalized (EAT) Intubation – An Awake Intubation Update. EMCrit Blog. Published on July 29, 2016. Available at [https://emcrit.org/emcrit/awake-intubation-update/ ].
Paix BR, Griggs WM. Emergency surgical cricothyroidotomy: 24 successful cases leading to a simple ‘scalpel-finger-tube’ method. Emerg Med Australas. 2012;24(1):23-30.
Scott Weingart. EMCrit Podcast 131 – Cricothyrotomy – Cut to Air: Emergency Surgical Airway. EMCrit Blog. Published on August 26, 2014. Accessed on May 16th 2018. Available at [https://emcrit.org/emcrit/surgical-airway/ ].
Drs. Helman and Dr. Weingart have no conflicts of interest to declare.
Other FOAMed Resources on Airway Pitfalls
First10EM on airway preparation
EMCrit on preoxygenation
EM Cases on preoxygenation and DSI
Rebel EM on hypotension kills
RESUS.ME on head rotation for mask ventilation
LiTFL on RSI in the shock patient
Rebel EM on dosing sedative low and paralytics high
EMCrit on Push-Dose Pressors
EMCrit on hemodynamic neutral intubation
LiTFL on awake intubation
Airway Jedi on indications for awake intubation
EMCrit on Rapid Sequence Awake – An Awake Intubation Update
EMCrit on Failed Intubation
Now test your knowledge with a quiz.



Hi
I’m Xan , an emergency physician from an EMS in the north Spain, Galiza.
“Aim for a MAP of 80 or SBP of 120-140”
About this….
What is your SBP target in a shocked TRAUMA patient?
I know resuscitate first and intubate second.
May you overpass the permissive hipotension for a while?
I like atot your foamed work.
Thanks