
This is EM Cases Episode 96 – Beyond ACLS Cardiac Arrest – Live from EMU Conference 2017 with Jordan Chenkin.
I had the privilege of speaking at Canada’s largest EM Conference, North York General’s Emergency Medicine Update Conference. This year they celebrated their 30th conference in Toronto and rather than give a standard plenary talk, we decided to do a live podcast. Jordan Chenkin (who heads up the University of Toronto EM POCUS program and who has taught at the EM Cases Course as well as many other EM conferences), joined me in discussing 3 areas where your cardiac arrest management can be optimized beyond the ACLS protocols: refractory ventricular fibrillation, optimized pulse checks and PEA arrest. In these 3 areas, we show videos of a code team performing the ACLS way and then contrasted that with videos of optimized approaches. This meant that a video format had to used for the podcast. So, we are excited to share the first ever video podcast on EM Cases!
Blog post by Anton Helman Month, May 2017
Cite this podcast as: Helman, A, Chenkin, J. Beyond ACLS Cardiac Arrest – Live from EMU Conference 2017. Emergency Medicine Cases. May, 2017. https://emergencymedicinecases.com/episode-99-highlights-emu-2017/. Accessed [date].
SHOCK REFRACTORY VF
1. Minimize the perishock pause
Stop chest compressions only to assess for defibrillation and to defibrillate.
Perishock pauses <20 s in the early resuscitation period are associated with survival to discharge when compared to episodes with peri-shock pause ≥40 s.
Tips to minimize the perishock pause:
- Pre-charge the defibrillator during chest compressions
- Count down before pausing for a shock so that the shock is delivered in between chest compressions and the hands come off the chest only momentarily
- Use a look-through monitor whereby the cardiac rhythm can be identified while chest compressions are ongoing
2. Dual Shock Therapy for Refractory Ventricular Fibrillation
Dual Shock Therapy (“double defib” or “double sequential defib”) involves defibrillating patients who are refractory to multiple defibrillations with 2 defibrillators at the same time or within seconds of each other, one with pads set up in the traditional anterior positions and the other set up with anterior-posterior pad positions.
A recent observational case series showed improved rates of ROSC with dual shock therapy with one patient surviving to hospital discharge.
An RCT in 1989 by Bardy randomized patients with refractory ventricular fibrillation to dual vs single shock therapy and found no significant difference in ROSC.
Despite the lack of definitive evidence that dual shock therapy improves survival, we recommend attempting it when other ![]() avenues have been exhausted in the patient with refractory ventricular fibrillation.
avenues have been exhausted in the patient with refractory ventricular fibrillation.
3. Stop Epinephrine after 3 doses or lower the dose
During refractory ventricular fibrillation and VF storm there is a huge catecholamine surge that![]() contributes to the refractoriness. Rather than adding more catecholamine with epinephrine, our experts recommend stopping the epinephrine after 3 doses or lowering the dose in ventricular fibrillation.
contributes to the refractoriness. Rather than adding more catecholamine with epinephrine, our experts recommend stopping the epinephrine after 3 doses or lowering the dose in ventricular fibrillation.
Some experts believe that the dose of 1mg every 3-5 minutes that is recommended in the guidelines is too high, is too frequently given and may be detrimental. Epinephrine, in the doses used in cardiac arrest, causes cerebral vasoconstriction that may impair tissue oxygenation, brain perfusion and compromise neurological recovery.
In most patients with ventricular fibrillation the primary cause is cardiac ischemia. Some experts believe that we should lower the dose of epinephrine in patients with ventricular fibrillation to minimize the vasoconstriction of the coronary arteries caused by epinephrine.
4. Block the catecholamine surge with esmolol
Esmolol is a fast acting B-blocker that increases the fibrillation threshold. Damaged myocardial cells are more sensitive to sympathetic tone, which esmolol blocks. No medication, including epinephrine has ever been shown to increase survival to hospital discharge, but esmolol has shown some promising results.
Esmolol was shown in a small study to double the rate of ROSC from about 1/3 of patients to 2/3 of patients, and to increase survival to hospital discharge with good neurological function from 11% to 50%. Larger studies are needed to confirm these findings, but so far the evidence looks promising.
Esmolol dosing in refractory VF:
500 mcg/kg IV push followed by infusion starting at 50 mcg/kg/min
![]() Update 2020: A randomized clinical trial demonstrated significant benefit of extracorporeal membrane oxygenation (ECMO) facilitated resuscitation in patients with out of hospital cardiac arrest and refractory ventricular fibrillation, when compared to standard ACLS. Abstract
Update 2020: A randomized clinical trial demonstrated significant benefit of extracorporeal membrane oxygenation (ECMO) facilitated resuscitation in patients with out of hospital cardiac arrest and refractory ventricular fibrillation, when compared to standard ACLS. Abstract
OPTIMIZING PULSE CHECKS & DETECTION OF ROSC
 Pulse checks are only needed if an organized rhythm is seen on the monitor.
Pulse checks are only needed if an organized rhythm is seen on the monitor.
Manual pulse checks have been shown to be insensitive, not specific and have poor inter-rater reliability. One study showed that rescuer pulse palpation was only 78% accurate. Even if a pulse is felt, this does not guarantee adequate perfusion to vital organs.
4 approaches to detecting ROSC and optimizing pulse checks can be considered:
1. POCUS: Have a dedicated experienced provider look on POCUS for a carotid pulse during chest compressions so that as soon as a pause in chest compressions to assess for cardiac rhythm occurs at the end of 2 minutes of compressions, the pulse can be rapidly assessed along with the cardiac rhythm in less than 5 seconds (as opposed to less than 10 seconds as recommended in the guidelines).
Or have a dedicated experienced provider look on cardiac POCUS in the epigastric for brisk cardiac activity.
2. Do not stop for a pulse check at all! Chest compressions should continue until:
- The end tidal CO2 monitor shows persistent elevations >30-40.
- An early established arterial line shows persistent DBP>30-40.
- Oxygen saturation from a finger probe shows a persistent wave form.
![]() Update 2017: International Federation of EM Consensus on POCUS for shock and cardiac arrest
Update 2017: International Federation of EM Consensus on POCUS for shock and cardiac arrest
PULSELESS ELECTRICAL ACTIVITY – PEA ARREST
The ACLS Guidelines continue to recommend running through the H’s and T’s in order to arrive at a specific diagnosis and guide treatment in PEA arrest. This approach may not be ideal because the H’s and T’s are difficult to remember in the heat of a stressful resuscitation and some of the H’s and T’s are rare causes of PEA (hypoxia, hypokalemia and hypoglycemia) or are obvious (hypoxia, hypothermia). In contrast, a novel approach to PEA arrest focuses on the more likely diagnoses that require immediate treatment beyond your C-A-Bs to achieve ROSC.
This way of thinking about PEA combines initial ECG morphology with the clinical scenario to guide the clinician to the most likely causes, and offer further diagnostic certainty using point of care ultrasound (POCUS). The first key step is to distinguish between narrow complex and wide complex PEA, with POCUS being used to help differentiate the causes of narrow complex PEA in particular.
Ideally, a designated team member provides the specific POCUS role independent of the other team members.
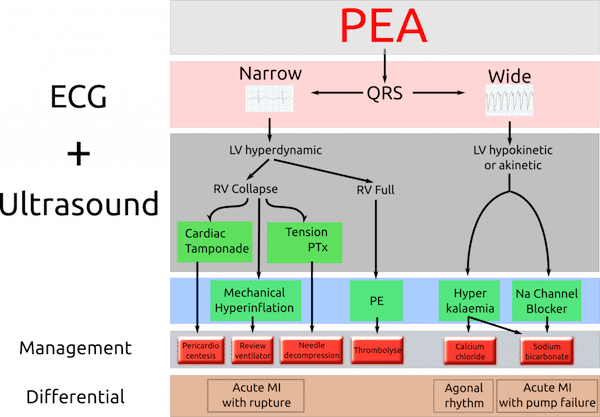
From Adelaide Emergency Physicians Education Resource
For an evidence-based critique of this approach to PEA arrest visit Rory Spiegel’s EM Nerd blog
Adjust Epinephrine Dose
If you see a vigorous heart on POCUS, rather than administer 1 amp of crash cart epinephrine, consider push dose epinephrine guided by blood pressure. Take a 10 ml syringe with 9 ml of normal saline. Into this syringe, draw up 1 ml of epinephrine from the cardiac amp (amp contains Epinephrine 100 mcg/ml). Now you have 10 mls of Epinephrine 10 mcg/ml. Administer 0.5-2 ml every 1-5 minutes (5-20 mcg). A titrated epinephrine infusion is another option.
Scott Weingart describes titrating epinephrine in cardiac arrest to hemodynamic parameters in this EMCrit podcast. Titrating to diastolic BP, as described in the Paradis study in JAMA requires early placement of an arterial line during ongoing chest compressions.
A special thank you to the actors in this episode video: Craig Brick, MD, Puneet Kapur, MD, Sue Spina, RN and Dean Maroney, RN.
![]() For more on ACLS Guidelines on EM Cases:
For more on ACLS Guidelines on EM Cases:
Episode 12 Part 1: ACLS Guidelines – What’s New & Controversial
Episode 12 Part 2: ACLS Guidelines – Atropine, Adenosine & Therapeutic Hypothermia
Episode 71 ACLS Guidelines 2015 – Cardiac Arrest Controversies Part 1
Episode 72 ACLS Guidelines 2015 Post Arrest Care
Dr. Helman and Dr. Chenkin have no conflicts of interest to declare.
References
Cheskes S1, Schmicker RH, et al. Perishock pause: an independent predictor of survival from out-of-hospital shockable cardiac arrest. Circulation. 2011 Jul 5;124(1):58-66.
Hagihara A, et al. Prehospital Epinephrine Use and Survival Among Patients With Out-of-Hospital Cardiac Arrest. JAMA. 2012;307(11):1161-1168
Driver BE, Debaty G, Plummer DW, Smith SW. Use of esmolol after failure of standard cardiopulmonary resuscitation to treat patients with refractory ventricular fibrillation. Resuscitation. 2014;85(10):1337-41.
Bardy GH, Ivey TD, Allen MD, Johnson G, Greene HL. Prospective comparison of sequential pulse and single pulse defibrillation with use of two different clinically available systems. J Am Coll Cardiol. 1989;14(1):165-71.
Eckstein M, Hatch L, Malleck J, Mcclung C, Henderson SO. End-tidal CO2 as a predictor of survival in out-of-hospital cardiac arrest. Prehosp Disaster Med. 2011;26(3):148-50.
Paradis, N, Coronary Perfusion Pressure and the Return of Spontaneous Circulation in Human Cardiopulmonary Resuscitation. JAMA. American Medical Association (AMA), 1990; February 23.
Scott Weingart. EMCrit Podcast 130 – Hemodynamic-Directed Dosing of Epinephrine for Cardiac Arrest. EMCrit Blog. Published on August 10, 2014. Available at [https://emcrit.org/podcasts/hemodynamic-directed-dosing-epinephrine/
Cheskes S, Schmicker RH, Verbeek PR, et al. The impact of peri-shock pause on survival from out-of-hospital shockable cardiac arrest during the Resuscitation Outcomes Consortium PRIMED trial. Resuscitation. 2014;85(3):336-42.
Littmann L, Bustin DJ, Haley MW. A simplified and structured teaching tool for the evaluation and management of pulseless electrical activity. Med Princ Pract. 2014;23(1):1-6.
Other FOAMed Resources on cardiac arrest care beyond ACLS
Scott Weingart. EMCrit Podcast 130 – Hemodynamic-Directed Dosing of Epinephrine for Cardiac Arrest. EMCrit Blog. Published on August 10, 2014. Available at https://emcrit.org/podcasts/hemodynamic-directed-dosing-epinephrine/
Scott Weingart. Podcast 191 – Cardiac Arrest Update. EMCrit Blog. Published on January 23, 2017. Available at https://emcrit.org/podcasts/cardiac-arrest-update/
The REASON Trial: POCUS in Cardiac Arrest at RebelEM
A Myth Revisited: Epinephrine for Cardiac Arrest at emDocs
A new PEA diagnostic algorithm: ECG and ultrasound at Adelaide Emergency Physicians EDucation Resources



I work at a very rural hospital in Wyoming. We do a good job of achieving ROSC but after the patient is shipped to the tertiary ctr they are not neurologically salvageable. I know capnography is helpful in predicting ROSC but do we have any surrogates to help guide post ROSC. I didn’t know if anyone has looked at prolonged pH etc.
I wanted to thank you for including the challenges small/rural providers face in your education.
Hi Adam, I admire the work that rural emergency providers like yourself do. Helpful surrogates to guide post ROSC include rough indicators of organ perfusion like base deficit, lactate, urine output etc. I don’t know of any studies in particular but will look into it.
Hello! Awesome podcast and really great information! Im a young doctor in sweden, working mostly with ortho. I have a question surrounding the perishock pause, how do you handle rythm analysis since you’d want to eliminate as much of the perishock pause as possibl, thx for any answer! /Per