
In this ECG Cases blog we look at 9 patients who presented with features suggestive of aortic dissection. How does the ECG change your diagnostic approach?
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. August 2022
Nine patients presented with clinical features suggestive of aortic dissection. How does the ECG change your diagnostic approach?
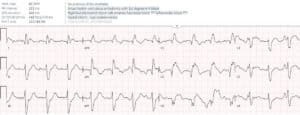
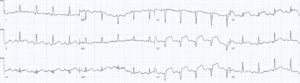
Case 1: 75 year old, history of hypertension, with 12 hours of back pressure radiating to chest and bilateral arms with diaphoresis. Normal vitals and exam




The ECG in aortic dissection
Aortic dissection is a rare but life-threatening emergency, which has a high rate of delayed diagnosis because the symptoms, ECG and lab findings are nonspecific and overlap with far more common emergencies including ACS or PE. As the Canadian practice guidelines summarize, the evaluation of patients presenting with possible aortic dissection starts with a pre-test probability assessment to guide decision-making.[1] This includes 1) high-risk conditions, eg connective tissue disease, aortic aneurysm, aortic valve disease or recent surgery; 2) high-risk pain features, eg sudden, severe, ripping, migrating, radiating; 3) high-risk exam findings: pulse deficit (not just a blood pressure differential), neurological deficit, new aortic insufficiency murmur, hypotension or pericardial effusion; and 4) considering alternate diagnoses.
The ECG is important for considering alternate diagnoses, but this is complicated by the spectrum of changes. The ECG can be completely normal in aortic dissection, show chronic LVH, or show a variety of ischemic ST/T wave changes—including acute coronary occlusion secondary to aortic dissection. As the European dissection guidelines summarize, “In the presence of a complete coronary obstruction, the ECG may show ST-segment elevation myocardial infarction. Also, myocardial ischemia may be exacerbated by acute aortic regurgitation, hypertension or hypotension, and shock in patients with or without pre-existing coronary artery disease. This may explain the observation that approximately 10% of patients presenting with acute Type B aortic dissection have ECG signs of myocardial ischemia.[2] How do we incorporate the ECG in the assessment of patients with features suggestive of aortic dissection?
- ECG diagnostic of acute coronary occlusion is highly unlikely to be secondary to aortic dissection, and CT scans delay reperfusion
While ECG abnormalities in patients with dissection are common, those mimicking acute coronary occlusion are not: less than 10% of type A aortic dissections have new Q waves or ST elevation [3], making it an uncommon occurrence in a rare disease. This should not distract from a far more likely and equally time-sensitive emergency: in a study of more than 1,500 patients with STEMI, only 0.51% were secondary to aortic dissection.[4] So with an ECG diagnostic of acute coronary occlusion, looking for a rare secondary cause will cause patient harm in more than 99% of cases. In study of more than 400 patients with STEMI, 11% had prolonged door-to-balloon time because of a CT scan looking for stroke, PE or aortic dissection; only 4% of scans changed management by identifying stroke, while none found an aortic dissection [5]. The risk of delayed reperfusion is greater for patients whose ECGs are diagnostic for Occlusion MI but don’t meet STEMI criteria, STEMI(-)OMI.
As the American guidelines on aortic dissection note, “the presence of a single high-risk feature (ie, high-risk condition, pain, or physical examination) may trigger immediate concern for acute aortic dissection; however, other diagnostic considerations may exist”, and an ECG consistent with STEMI in a patient with only one high risk feature is “likely primary ACS: in absence of other perfusion deficits, strongly consider immediate coronary reperfusion therapy.”[6] The newer European [2] and Canadian guidelines [1] put the ECG higher on the algorithm as part of the initial clinical assessment, with STEMI leading to immediate angiography even before determining pre-test probability of aortic dissection because the ECG has identified an alternate diagnosis.
- Non-diagnostic ECG: serial ECG, POCUS, labs, +/- CT based on pretest probability
While the major pitfall in ECGs diagnostic of acute coronary occlusion is delaying reperfusion to look for aortic dissection, the major pitfall in non-diagnostic ECGs is not considering aortic dissection in the presence of high-risk features.
Nearly a third of aortic dissections have ECGs that are normal, which might raise suspicion in a patient with sudden/severe pain (though dynamic or electrocardiographically silent Occlusion MI is still more likely). A quarter of patients with aortic dissection have an ECG showing LVH, with secondary repolarization abnormalities that might be misinterpreted as primary ischemic changes. Aortic dissection can also cause diffuse subendocardial ischemia through shock, tamponade, or left main stenosis, and is on the differential of diffuse ST depression with reciprocal ST elevation in aVR [7]
As none of these ECG findings are specific for aortic dissection or an alternate diagnosis, further tests are required based on pre-test probability. POCUS can complement ECG at the bedside—by identifying regional wall motion abnormalities from Occlusion MI[8], or indirect and direct signs of aortic dissection (dilated aortic root, intimal flap, pericardial effusion, aortic regurgitation)[9]
Back to the cases
Case 1: high-risk pain only but STEMI(+)OMI unlikely from aortic dissection, reperfusion delayed by CT
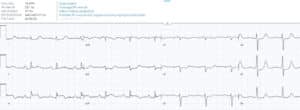
- Heart rate/rhythm: normal sinus rhythm
- Electrical conduction: normal intervals
- Axis: normal axis
- R-wave: delayed R wave progression
- Tall/small voltages: normal voltages
- ST/T changes: inferior STE with reciprocal STD in I/aVL and precordial STD max V1-4
Impression: inferoposterior STEMI(+)OMI with back pain. The patient had a CT chest because of back pain: no dissection. Then cath lab activated: 100% RCA occlusion, with prolonged ECG-to-Activation time. First trop 1500ng/L (normal <16 in females and <26 in males) and peak 100,000. Discharge ECG had inferior reperfusion T wave inversion with reciprocally tall T waves, and improvement of anterior ST depression.

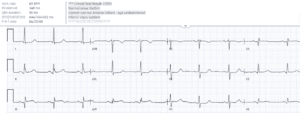
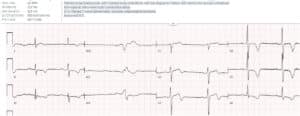
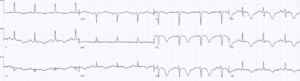
- H: normal sinus rhythm
- E: normal conduction
- A: normal axis
- R: new early R wave progression with R>S in V2
- T: normal voltages
- S: new STE in III/aVF with Q in III, reciprocal STD in I/aVL and STD in V2-3
Impression: infero-posterior OMI. CTA done because of BP difference: no dissection. Cath lab activation, with prolonged ECG-to-Activation time: 99% RCA occlusion. First trop 250ng/L and peak 14,000. Discharge ECG had inferior Q wave and reperfusion T wave inversion:
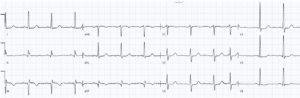
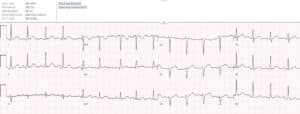
- H: sinus tach
- E: normal conduction
- A: normal axis
- R: normal R wave
- T: normal voltages
- S: no ST/T changes
Impression: nondiagnostic ECG in patient with acute chest pain and hypertension. Had nitro for BP control and CT chest: no dissection. Pain improved, first trop 150ng/L and repeat ECG:
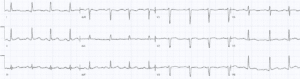
Anterior T waves have diminished in size with mild terminal inversion suggesting reperfusion. Then developed recurring chest pain:
Anterior ST elevation without reciprocal change. Cath lab activated: 99% mid LAD occlusion. Peak trop 8,000ng/L. Discharge ECG had antero-inferior reperfusion T wave inversion:
Case 4: stroke + proximal LAD occlusion: CT identified stroke and ruled out dissection, then cath lab for reperfusion
- H: normal sinus rhythm
- E: first degree AV block, RBBB and LAFB
- A: left axis from LAFB
- R: early R wave from RBBB
- T: normal voltages
- S: anterolateral ST elevation with Q waves, and reciprocal inferior ST depression
Impression: RBBB + LAFB + anterolateral STE = proximal LAD occlusion with high mortality rate. The associated stroke could be from aortic dissection causing both, or from subacute LAD occlusion causing embolic stroke. Stat cardiology consult to plan CT and cath: CT head revealed MCA embolic stroke, CT chest found no dissection, and then taken to cath lab: proximal LAD occlusion, then cardiac arrest
- H: sinus bradycardia
- E: normal conduction
- A: normal axis
- R: normal R wave
- T: normal voltages
- S: primary T wave inversion V2-6 and inferiorly
Impression: ECG appearance of Wellens but patient had active chest/back pain and abnormal vitals. Cath lab activated: normal coronaries but type A dissection. Repeat ECG had resolution of changes:

- H: sinus bradycardia
- E: borderline first degree AV block, otherwise normal conduction
- A: normal axis
- R: normal R wave
- T: tall voltages from LVH
- S: V4-6 ST depression and asymmetric T wave inversion, discordant and proportional to LVH
Impression: LVH with secondary ST/T changes that can be mistaken for primary ischemic changes, in patient with severe chest pain. Had cath lab activated but coronaries were normal, then diagnosed with type B aortic dissection.
- H: normal sinus rhythm
- E: normal conduction
- A: physiological left axis
- R: normal R wave progression except for V2, likely misplaced
- T: normal voltages
- S: mild concave inferolateral STE
Impression: pericarditis as diagnosis of exclusion, but elderly patient with back/chest pain. Treated with aspirin, serial troponin rose from 30ng/L to 60ng/L, leading to a consideration of myocarditis. But back pain increased, and CT revealed type A aortic dissection with small pericardial effusion.
- Heart rate/rhythm: atrial fibrillation
- Electrical conduction: normal intervals
- Axis: normal
- R-wave progression: normal
- Tall/small voltages: normal voltages
- ST/T: mild ST concave elevation V2-5, possible hyperacute T waves II/aVF, no reciprocal changes
Impression: syncope and shock with ECG suggesting anterior STEMI but no pulmonary edema from cardiogenic shock. Had cath lab activated, normal coronaries but found type A dissection complicated by large pericardial effusion. Then cardiac arrest.
- H: sinus bradycardia
- E: normal conduction
- A: normal axis
- R: normal R wave progression
- T: normal voltages
- S: mild terminal T wave inversion in V2
Impression: ECG could mimic subtle Wellens, but patient had ongoing severe back pain and low blood pressure. POCUS showed a flap in the abdominal aorta, then a stat CT chest revealed type A dissection.
Take home points for ECG in aortic dissection
- The ECG in aortic dissection can range from normal, to chronic LVH, to acute ST/T changes
- ECGs diagnostic of acute coronary occlusion are unlikely to be secondary to aortic dissection, and CT scans to rule out aortic dissection lead to reperfusion delays
- Non-diagnostic ECGs require other tests (including POCUS) guided by pre-test probability
References for ECG Cases 34 – ECG Interpretation in Aortic Dissection
- Ohle R, Yana JW, Yadav K, et al. Diagnosing acute aortic syndrome: a Canadian clinical practice guideline. CMAJ 2020 July 20;192:E832-43
- 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J 2014;35:2873-2926
- Costin NI, Korach A, Loor G, et al. Patients with type A acute aortic dissection presenting with an abnormal electrocardiogram. Ann Thor Surg 2018;105-92-9
- Zhu Q, Tai S, Tang L, et al. STEMI could be the primary presentation of acute aortic dissection. Am J Emerg Med 2017 Nov;35(11):1713-1717
- Armstrong EJ, Kulkarni AR, Hoffmayer KS, et al. Delaying primary percutaneous coronary intervention for computed tomographic scans in the emergency department. Am J Cardiol 2012 Aug; 10(3):345-349
- 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease. Circ 2010;121:e266-e369
- Kosuge M, Kazuo K, Uchida K, et al. Clinical implications of electrocardiograms for patients with type A acute aortic dissection. Circ J 2017;81:1254-1260
- Xu C, Lelendez A, Nguyen T, et al. Point-of-care ultrasound may expedite diagnosis and revascularization of occult occlusive myocardial infarction. Am J Emerg Med 2022 Aug;58:186-191
- Pare JR, Lui R, Moore CL et al. Emergency physician focused cardiac ultrasound improves diagnosis of ascending aortic dissection. Am J Emerg Med 2016;34:486-492



Leave A Comment