
Topics in this EM Quick Hits podcast
Anand Swaminathan on limitations and practical tips on intraosseus access (0:58)
Tahara Bhate QI corner on missed ectopic pregnancy (11:38)
Sarah Reid from EM Cases Summit on oxygen saturation monitoring in bronchiolitis and management of infant gastro-esophageal reflux (22:35)
Brit Long on the value of rectal exam in diagnosis of cauda equina syndrome (28:40)
Hans Rosenberg & Ariel Hendin on withdrawal of life-sustaining care in the ED (32:26)
Podcast: Play in new window | Download (Duration: 42:57 — 39.4MB)
Subscribe: Apple Podcasts
Podcast production, editing and sound design by Anton Helman
Podcast content, written summary & blog post by Anand Swaminathan, Michelle Klaiman, Hans Rosenberg, Anna MacDonald & Justin Morgenstern, edited by Anton Helman
Cite this podcast as: Helman, A. Swaminathan, A. Klaiman, M. Rosenberg, H. MacDonald A, Morgenstern J. EM Quick Hits 1 – Massive PE, Gabapentin for Alcohol Withdrawal, Dental Avulsions, Pediatric Eye Exam, Best Resuscitation Fluid. Emergency Medicine Cases. January, 2019. https://emergencymedicinecases.com/em-quick-hits-january-2019/. Accessed August 10, 2026.
Intraosseous (IO) access limitations and tips
Limitations of IO access include:
- Placing an IO in a bone with a proximal fracture, a previous IO placement attempt or any circulatory compromise proximal to the site is contraindicated
- Blood work drawn from an IO are genrally not accurate, so once the patient has been resuscitated with the IO, intravenous blood draws are recommended
- Dislodgement is common; it is best to use the stabilizer that comes with the IO kit; if the kit does not have a stabilizer, stack lots of gauze on both sides of the IO needle and tape it down
- IOs are only suitable for term infants > 3kg weight; avoid IOs in premies
Best site for IO?
- While proximal humerus site portents faster infusion rates than proximal tibia site, the main limitation of the proximal humerus site is that the arm must be held in internal rotation to avoid dislodgement of the IO
- Proximal tibia may be easier to landmark than proximal humerus
- Other sites include distal tibia, distal femur and sternum but are uncommonly employed in EDs
Needle size?
- There are 3 weight-based IO needle sizes, but most experts prefer to choose the needle based on the estimated distance from skin to bone (ie amount of soft tissue)
- It is better to overestimate than to underestimate the needle size based on distance from skin to bone
- Sá RA, Melo CL, Dantas RB, Delfim LV. Vascular access through the intraosseous route in pediatric emergencies. Rev Bras Ter Intensiva. 2012 Dec;24(4):407-14.
- Luck, R. Haines, C. & Mull, C. (2010). Intraosseous Access. The Journal of Emergency Medicine. 39(4), 468-475.
- Ngo, A. et.al. (2009). Intraosseous vascular access in adults using the EZ-IO in an emergency department. International Journal of Emergency Medicine. 2, 155-160.
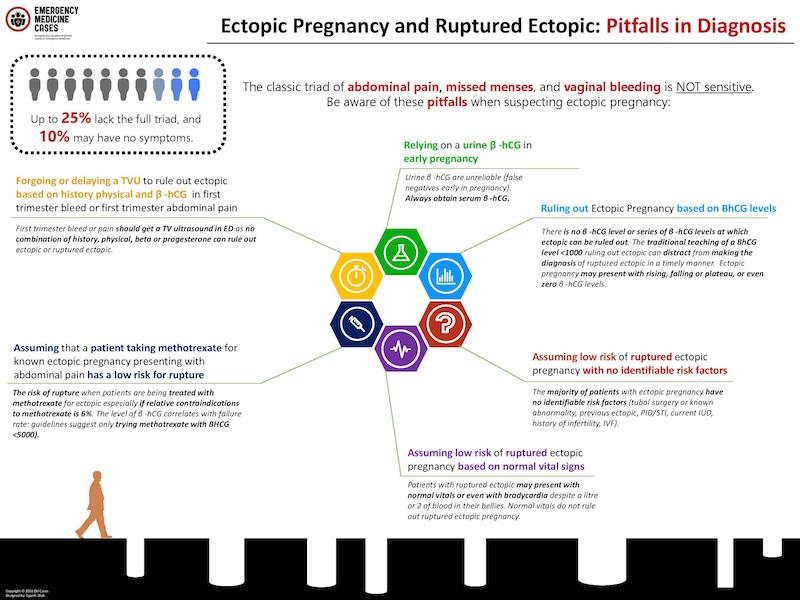
Missed ectopic pregnancy
- Ectopic pregnancy presents with the classic triad of pain, amenorrhea, and vaginal bleeding only about 50% of the time
- There is no combination of history, physical and blood work that definitively rules out ectopic pregnancy (there are even case reports of undetectable serum BhCG with confirmed ruptured ectopic pregnancy!)
- Despite a meta-analysis of studies of ED point of care pelvic ultrasound (PoCUS) showing a sensitivity of 99.3% and a NPV of 99.6% for the diagnosis of ectopic pregnancy there remains inter-operator skill variability and cases are missed; consider a quality assurance program for PoCUS, as recommended by CAEP, such as an archive and review system that flags and addresses discrepancies for your ED
- Use of PoCUS for the diagnosis of ectopic pregnancy may result in shorter length of stay in the ED and faster time to definitive treatment for ruptured ectopic when compared to radiology-based ultrasound alone based on the literature
Dr. Catherine Varner’s Best Case Ever reviewing 6 pitfalls in diagnosis of ectopic pregnancy
Episode 23: Vaginal Bleeding in Early Pregnancy
- Stein JC, Wang R, Adler N, Boscardin J, Jacoby VL, Won G, et al. Emergency physician ultrasonography for evaluating patients at risk for ectopic pregnancy: a meta-analysis. Ann Emerg Med. 2010;56(6):674-83.
- Daniilidis A, Pantelis A, Makris V, Balaouras D, Vrachnis N. A unique case of ruptured ectopic pregnancy in a patient with negative preg-nancy test – a case report and brief review of the literature. Hippokratia. 2014 Jul-Sep;18(3):282-4.
- Stone BS, Muruganandan KM, Tonelli MM, Dugas JN, Verriet IE, Pare JR. Impact of point-of-care ultrasound on treatment time for ectopic pregnancy. Am J Emerg Med. 2021 Nov;49:226-232.
- Lewis D, Rang L, Kim D, Robichaud L, Kwan C, Pham C, Shefrin A, Ritcey B, Atkinson P, Woo M, Jelic T, Dallaire G, Henneberry R, Turner J, Andani R, Demsey R, Olszynski P. Recommendations for the use of point-of-care ultrasound (POCUS) by emergency physicians in Canada. CJEM. 2019 Nov;21(6):721-726.
Oxygen saturation monitoring in bronchiolitis
- There is in-hospital evidence to suggest that continuous monitoring may prolong length of stay, particularly if staff react to normal transient dips in oxygen saturation or changes in heart and respiratory rates with interventions such as restarting oxygen therapy
- Many healthy infants exhibit typical transient O2 saturation dips
- The rationale for respiratory monitoring is to detect episodes of apnea requiring intervention; in a study of 691 infants <6 months of age, only 2.7% had documented apnea, and all had risk criteria of either a previous apneic episode or young age (<1 month or <48 weeks post-conception in premature infants)
- Continuous respiratory monitoring is indicated for high-risk patients in the ED, primarily to detect apneic episodes, but are not necessary for the vast majority of patients with bronchiolitis
=>Bottom line: Continuous O2 saturation monitoring in stable infants with mild-moderate bronchiolitis is unnecessary and may lead to needless admissions, prolonged length of stay; spot checks are adequate
Ep 177 Bronchiolitis – Diagnostic Challenges and Management Pitfalls
- Friedman JN, Rieder MJ, Walton JM; Canadian Paediatric Society, Acute Care Committee, Drug Therapy and Hazardous Substances Committee. Bronchiolitis: Recommendations for diagnosis, monitoring and management of children one to 24 months of age. Paediatr Child Health. 2014 Nov;19(9):485-98.
- Schroeder AR, Marmor AK, Pantell RH, Newman TB. Impact of pulse oximetry and oxygen therapy on length of stay in bronchiolitis hospitalizations. Arch Pediatr Adolesc Med 2004;158(6):527-30.
- Willwerth BM, Harper MB, Greenes DS. Identifying hospitalized infants who have bronchiolitis and are at high risk for apnea. Ann Emerg Med 2006;48(4):441-7.
- Hunt CE, Corwin MJ, Lister G, et al. Longitudinal assessment of hemoglobin oxygen saturation in healthy infants during the first 6 months of age. Collaborative Home Infant Monitoring Evaluation (CHIME) Study Group. J Pediatr 1999;135(5):580-6.
- Poets A, Urschitz MS, Poets CF. Intermittent hypoxia in supine versus side position in term neonates. Pediatr Res 2009;65(6):654-6.
Treatment of infant gastroesophageal reflux (GER)
- First line treatments include avoiding overfeeding and thickened feeds
- Second line treatment includes 2-4 weeks of a protein hydrolysate or amino acid based formula or, in breastfed infants, elimination of cow’s milk in maternal diet
- Third line treatment includes 4-8 week trial of acid suppression medication then wean if symptoms improved (with pediatric GI referral where available)
=>Bottom line: Anti-reflux medications should not be prescribed as a first line treatment for infants with GER in the ED
Parent checklist for reflux in infants
- Rosen R, Vandenplas Y, Singendonk M, Cabana M, DiLorenzo C, Gottrand F, Gupta S, Langendam M, Staiano A, Thapar N, Tipnis N, Tabbers M. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 2018 Mar;66(3):516-554.
The value of rectal tone assessment in diagnosing cauda equina syndrome (CES)
- The rectal exam primarily tests S2-S4 and includes the skin exam, superficial anal reflex/anal wink and DRE
- DRE with evaluation of rectal tone is not reliable or sensitive in assessing S2-S4 function
- 2015 study assessed provider ability to accurately detect decreased rectal tone on a simulator and found an overall correct assessment of 64%.
- 2022 meta-analysis of 6 studies with 741 patients with CES compared DRE to MRI found anal tone had a sensitivity of 23-53%, anal squeeze had a sensitivity of 29%, and anal reflexes had a sensitivity of 38% for CES
- If concerned about CES, perform focused history and examination evaluating L2-sacral nerve root function; ask about urinary changes (retention and incontinence), defecation changes (constipation and/or incontinence), sexual function changes, and saddle or anal sensory changes; sensory loss in a dermatomal pattern, saddle anesthesia, ankle/knee reflex loss and bilateral sciatica are concerning
=>Bottom line: rectal tone has a wide inter-observer variability and poor accuracy for the diagnosis of cauda equina syndrome and is unlikely to alter pre-test probability for the diagnosis of cauda equina syndrome
- Long B, Koyfman A, Gottlieb M. Evaluation and management of cauda equina syndrome in the emergency department. Am J Emerg Med. 2020 Jan;38(1):143-148.
- Sherlock KE, Turner W, Elsayed S, Bagouri M, Baha L, Boszczyk BM, McNally D. The Evaluation of Digital Rectal Examination for Assessment of Anal Tone in Suspected Cauda Equina Syndrome. Spine (Phila Pa 1976). 2015 Aug 1;40(15):1213-8.
- Tabrah J, Wilson N, Phillips D, Böhning D. Can digital rectal examination be used to detect cauda equina compression in people presenting with acute cauda equina syndrome? A systematic review and meta-analysis of diagnostic test accuracy studies. Musculoskelet Sci Pract. 2022 Apr;58:102523.
- Gooding BW, Higgins MA, Calthorpe DA. Does rectal examination have any value in the clinical diagnosis of cauda equina syndrome? Br J Neurosurg. 2013 Apr;27(2):156-9.
- Angus M, Curtis-Lopez CM, Carrasco R, et al. Determination of potential risk characteristics for cauda equina compression in emergency department patients presenting with atraumatic back pain: a 4-year retrospective cohort analysis within a tertiary referral neurosciences centre. Emerg Med J. 2021 Oct 12:emermed-2020-210540.
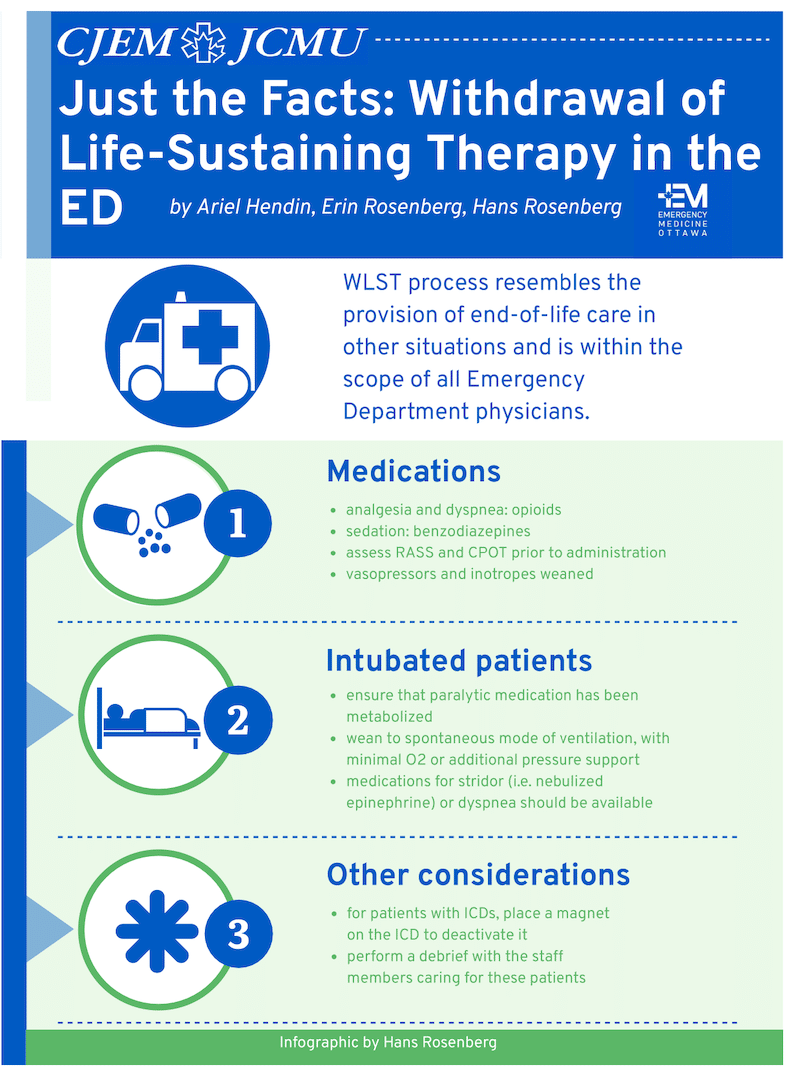
Withdrawal of life-sustaining therapy in the ED
- Withdrawal of life-sustaining therapy is the process by which therapies that support or replace vital organ function (eg. hemodialysis, mechanical ventilation, vasopressors) are discontinued
- Withdrawal of life-sustaining therapy is often recommended when it is clear that the expected outcome from ongoing life-sustaining therapy and other treatments would not be acceptable for the patient
- The CAEP 2020 statement states that withdrawal of life-sustaining therapy in the ED for patients with severe brain injury should only be offered if ongoing care is inconsistent with the patient’s wishes, if injuries render the patient significantly physiologically unstable, or if the patient has other comorbidities that would make it inappropriate for them to receive ongoing ICU care regardless
- Patients and their families should be offered organ donation which is seldom done
- Friedman JN, Rieder MJ, Walton JM; Canadian Paediatric Society, Acute Care Committee, Drug Therapy and Hazardous Substances Committee. Bronchiolitis: Recommendations for diagnosis, monitoring and management of children one to 24 months of age. Paediatr Child Health. 2014 Nov;19(9):485-98.
- Healey A, Leeies M, Hrymak C, Chochinov A, Grunau B, Pau- novic B, et al. CAEP Position statement—management of dev- astating brain injuries in the emergency department: enhancing neuroprognostication and maintaining the opportunity for organ and tissue donation. Can J Emerg Med. 2020;22(5):658–60.
-
Hendin A, Rosenberg E, Rosenberg H. Just the facts: withdrawal of life-sustaining therapy in the ED. CJEM. 2022 Jun;24(4):362-365.
None of the authors have any conflicts of interest to declare



Great Quick Hits episode, thanks so much! I’m an EM and palliative care physician in the US, and just wanted to offer one more pearl regarding de-escalation or withdrawal of life-prolonging treatment:
We often focus primarily on extubation in these situations, and I think the episode and infographic do a good job of hitting the highlights of how to approach that. However, depending upon the circumstances, removal of respiratory support can run a high risk of uncontrolled end of life symptoms, particularly dyspnea. If the patient is also on pressors, we generally recommend weaning and discontinuing those first, as hypotension/shock is generally significantly less symptomatic than respiratory failure is. In many cases you can facilitate a comfortable end of life by discontinuing pressors alone, and won’t have to run the risk of uncontrolled symptoms during and after extubation. So, if you have the option, try weaning and discontinuing the hemodynamic support and then reassessing, before focusing on extubation.
Brian Gacioch