
In this ECG Cases blog we review pitfalls and pearls for stable narrow complex tachycardias, including identifying secondary tachycardias and differentiating primary tachycardias
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. June 2026
8 patients presented with stable narrow complex tachycardias. Which will respond to ACLS algorithm and which require different treatments?
Case 1: 70 year old with vomiting
–
Case 2: 40 year old with palpitations
–
Case 3: 40 year old with palpitations
–
Case 4: 70 year old with chest pain
–
Case 5: 70 year old, history of AF, with few weeks shortness of breath

–
Case 6: 75 year old, previously healthy, with sudden palpitations
–
Case 7: 55 year old with weakness for a few days
–
Case 8: 85 year old with sudden palpitations. Initial computer interpretation ‘SVT’
–
Stable narrow complex tachycardias
This is the final in a series of blog posts on the pitfalls of ACLS algorithms for adults with a pulse – including pitfalls in ECG acquisition, ECG interpretation, and ECG application. Previous posts looked at the bradycardia algorithm including unstable bradycardia and stable bradycardia; then the tachycardia algorithm starting with unstable tachycardia and stable wide complex tachycardia, and now stable narrow complex tachycardia.
The ACLS approach to stable narrow complex tachycardia is simple: block the AV node through Valsalva maneuvers or medications such as adenosine, calcium channel blockers or beta-blockers. As with other ACLS algorithms, this assumes the patient has a primary arrhythmia. But in a CJEM study on narrow complex tachycardias ≥ 130bpm in the ED, a quarter were sinus tachycardia and half were atrial fibrillation of which a large minority had secondary causes. As a result, 45% of narrow complex tachycardias were secondary to underlying causes (eg infections, heart failure, bleeding or metabolic disorders) which will be harmed by rate control.[1] Conversely, the majority of atrial flutter and SVT (AVNRT/AVRT) were primary arrhythmias that respond well to initial ACLS algorithms, but need to be further differentiated.
Differentiating narrow complex tachycardias seems simple: AF if irregular, sinus if P waves, flutter if flutter waves and SVT (AVRT/AVNRT) if none. But this can be challenging at rapid rates. The same CJEM study found correct rhythm identification by emergency physicians decreased from 95% for AF to 90% for sinus tach, to 81% for SVT, to 61% for AFL.[1] This is compounded by computer interpretation that often overcalls AF (when it’s actually just artifact, sinus arrhythmia or PACs), and undercalls AFL (labeling it as sinus tach or SVT when it’s actually AFL). These computer interpretation not only affect the treating emergency physician but also the blinded cardiologist who confirms the final ECG interpretation.[2]
This highlights a number of ACLS pitfalls for stable narrow complex tachycardias:
- Acquisition: is it actually a tachy-arrhythmia or just artifact
- Interpretation
- Is it narrow? Computers that miss flutter or retrograde P waves may false label these ECGs as ‘wide complex’
- Narrow and irregular: is it AF, or sinus (with irregularity from sinus arrhythmia, premature or blocked beat)?
- Narrow and regular: is it sinus, AFL, or SVT? Sinus has P waves upright in II/I, biphasic in V1. Typical flutter waves are inverted inferiorly and upright in V1. SVT usually has retrograde P waves buried in the QRS or right after (short RP, from typical AVNRT), or the RP may be long (atypical AVNRT, orthodromic AVRT, or atrial tachycardia)
- Application:
- Secondary cause: is there an underlying cause for the tachycardia that needs treatment, including for sinus tach and atrial fibrillation?
- Repeat ECG: this can reassess the rate improvement after treating secondary causes, reassess rate-related ST/T changes after treatment of primary or secondary tachy-arrhythmias, or reveal WPW accessory pathway after SVT cardioversion
- Follow up: if it’s a primary arrhythmia, does it need treatment on discharge (eg anticoagulation for AF/AFL) or follow up (eg ablation)
Back to the cases
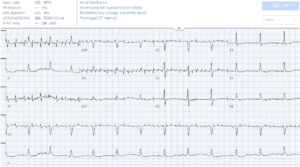
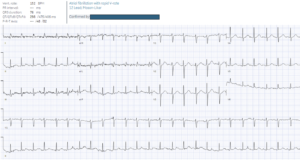
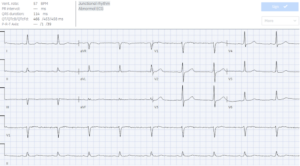
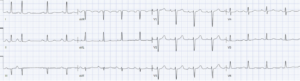
Case 1: 70 year old with vomiting. Artifact not AF
- Heart rate/rhythm: regular narrow complex rhythm, at normal rate, with upright P waves in the rhythm strip II = normal sinus. Artifact simulating AF, which spares lead II
- Electrical conduction: normal intervals
- Axis: normal
- R-wave progression: borderline early in V2
- Tall/small voltages: normal
- ST/T: normal
Impression: normal sinus with artifact, not AF. Treatment directed at underlying cause of vomiting. Repeat ECG no more artifact, still sinus rhythm (but the computer continues to miss the P waves)
–
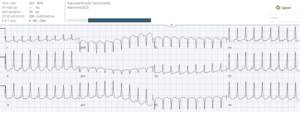
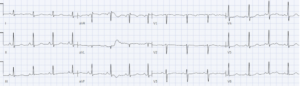
Case 2: 40 year old with palpitations. SVT with retrograde P wave, not wide complex tachycardia
- H: regular narrow complex tachycardia with retrograde P wave, short RP: AVNRT
- E: narrow not wide QRS
- A: normal
- R: normal
- T: normal
- S: normal
= SVT(AVNRT) not wide complex tachycardia. Post-cardioversion ECG was normal, and patient discharged with follow up for SVT.
–
Case 3: 40 year old with palpitations. AVRT with accessory pathway revealed on post-cardioversion ECG
- H: regular narrow complex tachycardia with long RP (seen best lead V1 and V3): atypical AVNRT vs orthodromic AVRT
- E: narrow QRS
- A: normal
- R: abnormal progression
- T: normal
- S: rate related diffuse STD
= AVNRT vs AVRT. Modified Valsalva failed, then cardioverted with adenosine:
- H: normal sinus
- E: short PR with delta wave
- A: normal
- R: early R wave in V2
- T: normal
- S: mild secondary STD V3
= WPW. Referred to electrophysiology clinic.
–
Case 4: 70 year old with chest pain. Sinus tach not AF
- H: narrow complex tachycardia with slight irregularity, with P waves of different morphologies before the QRS complexes = sinus tachycardia with PAC
- E: normal intervals
- A: normal axis
- R: normal
- T: normal
- S: normal
= sinus tachycardia, not AF, in patient with chest pain. Rather than rate control, the patient had CTPA that showed pulmonary embolism. Follow up ECG showed ongoing sinus tachycardia at slower rate

–
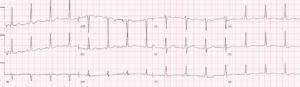
Case 5: 70 year old, history of AF, with few weeks shortness of breath. AF with RVR secondary to tamponade
- H: irregularly irregular narrow complex tachy without P waves = AF with rapid ventricular response
- E: normal QRS/QT
- A: normal axis
- R: borderline late
- T: diffuse small voltages
- S: no ST/T changes
Impression: AF/RVR with shortness of breath and low voltage. POCUS showed large pericardial effusion so initial treatment was fluids not rate control. Repeat ECG after pericardiocentesis showed larger voltages in the precordial leads:

–
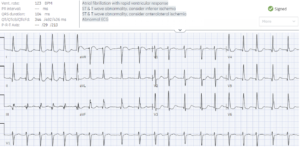
Case 6: 75 year old, previously healthy, with sudden palpitations. Primary AF with rate-related ST changes
- H: irregularly irregular narrow complex tachycardia without P waves = AF with RVR
- E: narrow QRS
- A: normal
- R: borderline early
- T: normal
- S: diffuse ST depression with reciprocal ST elevation in aVR
Impression: primary AF/RVR with rate-related ST changes. No secondary causes found, and post-cardioversion ECG showed normal sinus with resolution of ST changes:

–
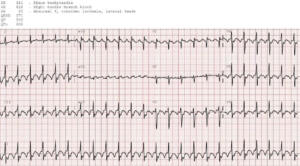
Case 7: 55 year old with weakness for a few days. Atrial flutter not sinus tachycardia with wide complex
- H: regular narrow complex tacychcardia with flutter waves (inverted inferior leads, upright in V1) = atrial flutter not sinus tach
- E: narrow not wide QRS, 2:1 conduction
- A: normal
- R: normal
- T: normal
- S: flutter waves, no ischemia
Impression: atrial flutter, not sinus tachy/RBBB/ischemia. No secondary causes found. Admitted for echo to exclude atrial thrombus then cardioversion: sinus rhythm (P wave upright in II and I, and inverted in V1 from high lead placement):
–
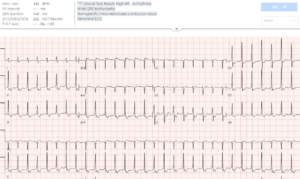
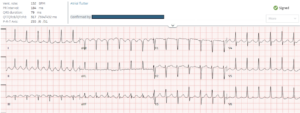
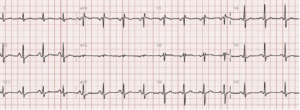
Case 8: 85 year old with sudden palpitations. Initial computer interpretation ‘SVT’. AFL not SVT
- H: regular narrow complex tachycardia with flutter waves (best seen inferior leads) = atrial flutter
- E: 2:1 conduction, narrow QRS
- A: normal
- R: normal
- T: normal
- S: no changes
Impression: sudden palpitations from atrial flutter, not SVT. Patient mistakenly diagnosed as SVT, electrically cardioverted into sinus rhythm and discharged without anticoagulation.
Returned next month with recurring atrial flutter and transient vision loss from TIA.
–
Take home points on Stable Narrow Complex Tachycardias
- Acquisition: is it actually a narrow complex tachycardia, or just artifact?
- Interpretation: If irregular, is it AF or sinus with another reason for irregularity? If regular, is it sinus (P wave upright in II, biphasic V1), flutter (typically inverted inferiorly and upright in V1), or SVT with buried/short PR (typical AVNRT) or long PR(atypical AVNRT, orthodromic AVRT, or atrial tachycardia)?
- Application: Is there a secondary cause that needs treatment? Does the repeat ECG show improvement from secondary cause treatment, resolution of rate-related changes, or reveal post-cardioversion accessory pathway? It’s a primary arrhythmia does if need anticoagulation or follow up?
More on Tachydysrhythmias with Amal Mattu and Paul Dorian on EM Cases
For live, highly interactive, and CME-accredited ECG courses to elevate your skills go to www.heartsECGcourse.com
References
- Linton JJ, Eagles C, Green MS, et al. Diagnosis and management of patients who present with narrow complex tachycardia in the emergency department. CJEM 2023;25: 303-313
- Anh D, Krishnan S, Bogun F. Accuracy of electrocardiogram interpretation by cardiologists in the setting of incorrect computer analysis. J Electrocardiol 2006;39(3):343-345

Leave A Comment